




Today’s VETgirl online veterinary continuing education guest blogger is Dr. Craig Clifford, DACVIM (Oncology), from Hope Veterinary Specialists, where he discusses new updates with canine lymphoma (e.g., lymphosarcoma). This content is previously published on Hope’s website.
Canine Lyphoma: Updates
If you’re wondering what’s new with canine lymphoma, read on! While “recipe” protocols were commonplace, lymphoma is no longer considered a one size fits all when it comes to treating these patients. That’s because there are newer molecular, immunologic and histologic diagnostics; therefore, the diagnosis and treatment of lymphoma is changing. Currently, decisions regarding which chemotherapeutic agents/protocols to be utilized is now based upon tumor grade, location, histologic subtype, and immunophenotype. Keep in mind that: Not all lymphomas are created equal!
Phenotyping
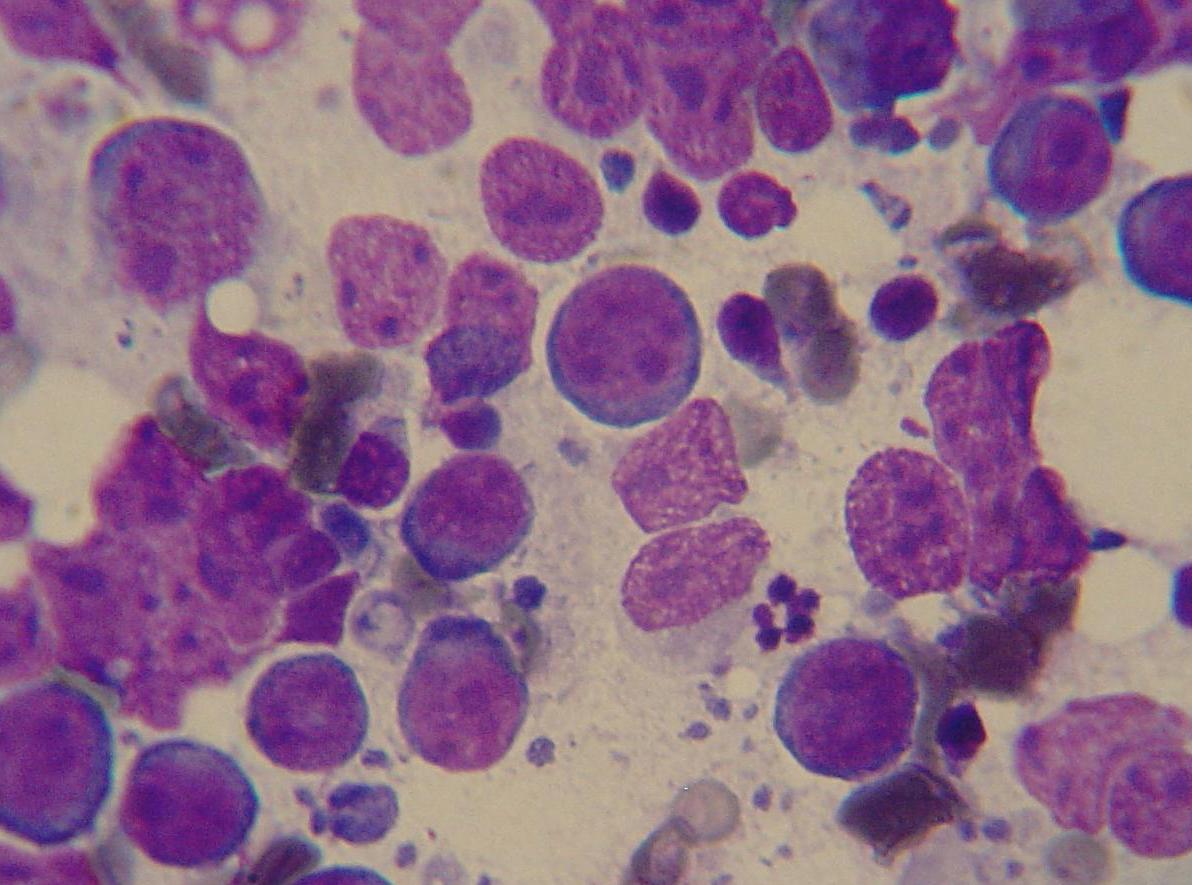
Canine lymphoma is divided into two basic phenotypes, B and T cell. Traditionally 2/3 of dogs with lymphoma are classified as B cell and 1/3 are T cell. Phenotyping of lymphoma patients can be achieved through a variety of tests including immunohistochemistry, immunocytochemistry (IHC), PARR and flow cytometry.1 In a recent study comparing Flow cytometry and Parr, using IHC as the “gold standard”, flow cytometry was found to be superior.1
Why Is Phenotype Important?
It well established that the T-cell phenotype carries a poor prognosis as compared to B cell lymphoma.2 The T cell phenotype is often associated with certain breeds including the boxer, golden retriever, Australian shepherd, Asian lap dogs and Siberian husky. T cell phenotype, interestingly, is also associated with certain anatomic forms including cutaneous (epitheliotropic), mediastinal, hepatic and gastrointestinal.
Based upon the limitation noted with standard protocols, oncologists have begun modifying protocols for T cell LSA. Support for this was based upon results of two studies. Beaver et al. evaluated the response rate of both B and T cell patients to a single dose of doxorubicin.2 Interstingly, the response of T cell dogs was ~50% vs ~100% for dogs with B cell LSA. Brodsky et al. evaluated the combination of L-asparagine, mechlorethamine, vincristine, procarbazine, and prednisone (L-MOPP) in dogs T-cell lymphoma.3 This protocol was associated with a complete remission rate of 78%, and overall survival 270 days, Interestingly, a subgroup of ~20% were alive at >900 days, which much longer than commonly observed.3 Cost, difficulty of administration and toxicity make this a somewhat challenging protocol to routinely utilize. In addition, epitheliotropic lymphoma (T cell) is commonly treated with lomustine (CCNU).4 Although, only 17% of dogs obtain a complete remission (CR), 61% obtain a partial remission (PR). The sum of this information has lead to several protocol modifications including increasing the number of alkylating agents in a protocol, utilizing l-asparaginase more frequently and substitution of CCNU for Doxrobucin.
Canine Indolent Lymphoma
High grade LSA generally represents nearly 80% of all LSA cases. In the past 10 years, we have identified a less aggressive histologic subtype of lymphoma deemed “indolent” or “low grade” lymphoma. This form can be either of B-Cell origin (CD79a+) including marginal zone lymphoma which appears to be the most common form involving lymph node and/or spleen, follicular lymphoma (lymph node), and mantle cell lymphoma (often occurring as a solitary splenic mass) or T cell origin (CD3+, CD45-), in which T-zone is the most common form.5-8
Patients with nodal indolent LSA often present with submandibular/cervical lymph node enlargement. The key difference vs that of high grade LSA resides in the history in which the lymphadenopathy has existed over a prolonged times frame of weeks to months, often with a waxing and waning of the disease. 5-7 The majority of patients are consider substage a with no clinical signs. The overall survival is significantly longer than that of “high grade” lymphoma. Interestingly, this is in the face of many patients received no chemotherapeutic agents. For cases with splenic involvement, the identification of a “mass effect” is most common.5-7
Unlike “high grade LSA, indolent LSA requires histopathology to definitively diagnose. Also, local therapy in the form of surgery (for stage I or II local lymph node involvement or splenic involvement) may provide long term control without the addition of chemotherapy. Various, less intense chemotherapy protocols have been anecdotally utilized and the use of chemotherapy is considered controversial. 5-7
Pathway to a Cure: “Novel Therapies”
Novel LSA Therapies:
Chemotherapy: Tanovea™ was discovered by Gilead Sciences, Inc., and licensed to VetDC for use in animal cancer, (previously known as VDC-1101). This agent was designed to preferentially target and attack cancer cells implicated in lymphoma. 8,9 The data from studies totaling well over 250 patients have shown Tanovea™ to be highly effective against LSA with a 60-80% overall response rate. Not surprisingly, responses are higher in naïve LSA vs relapse and in dogs with a B cell phenotype. Date suggests Tanovea™ is well-tolerated with a similar side effect profile as other commonly used agents. The administration is via the intravenous route with a 1mg/kg dosing every 3 weeks. Our hope, is that VetDC may obtain approval in mid 2016.
Monoclonal Antibodies
A monoclonal antibody (mAb) can be used to specifically bind to target cells or proteins and in turn stimulate the patient’s immune system to attack those targeted cells. In physician based oncology, monoclonal antibodies have been developed for the treatment of T and B cell Lymphoma. Cancer cell killing is thought to be via three mechanisms:
• Antibody-dependent cellular cytotoxicity (ADCC)
• Complement-mediated cytotoxicity (CMC)
• Induction of apoptosis (natural cell death)
Interestingly, normal lymphocytes are targeted as well but can be replenished, as stem cells within the bone marrow are not targeted. Similarly, plasma cells responsible for “memory” are not targeted.
Rituximab is one of the most well-known monoclonal antibodies and targets the CD20 antigen on the surface of B-lymphocytes. Rituximab was approved by the FDA in 1997 and is considered standard-of-care therapy in conjunction with chemotherapy for a number of human B-cell disorders. In dogs, expression of CD20 has been confirmed in B-cell lymphomas by immunohistochemistry using anti-human CD20 polyclonal antibodies that recognize the intracellular domains of CD20.1 Unfortunately, rituximab does not bind canine CD20. Development of canine monoclonal antibodies for treatment of B-cell and T-cell lymphomas would represent a massive advancement in the treatment of canine lymphoma.
Current Status of Monoclonal Antibodies
1. B-cell Monoclonal Antibody (MAb) (Aratana Therapeutics®): A caninized B-cell MAb (Blontress®) was fully licensed by the USDA in January 2015 as an aid in the treatment of canine B-cell lymphoma. This MAb is commercially marketed by Aratana Therapeutics®, Inc. Several studies have evaluated this monoclonal in dogs receiving condensed chemotherapy protocols and in each the addition of the monoclonal did provide a benefit. A recently completed prospective single arm study evaluated two cycle of standard CHOP + monoclonal. Data is maturing results will be likely be completed by mid 2016.
2. T-cell Mab (Aratana Therapeutics®): A caninized T-cell monoclonal antibody (Tactress®) was fully licensed by the USDA in January 2016 as an aid in the treatment of canine T-cell lymphoma. This monoclonal antibody is commercially marketed by Aratana Therapeutics, Inc. Two prospective multi-center, double-blind, randomized, placebo-controlled studies were recently completed to further evaluate the T-cell MAb in conjunction with cytotoxic chemotherapy for treatment of canine nodal T-cell lymphoma. Aratana completed an analysis of the results and T-cell MAb did not improve the progression free survival. The T cell monoclonal was used as part of an “experience” program in which all forms of T cell LSA were treated and data mining of this group is ongoing to determine subgroup efficacy.
3. Anti-CD20 Monoclonal Antibody (Elanco)
The generation and characterization of an anti-CD20 antibody intended as a candidate treatment for canine B-cell lymphoma has recently been described.10 A panel of anti-canine CD20 monoclonal antibodies was generated using a mouse hybridoma approach and specifically monoclonal antibody 1E4 was selected for construction of a canine chimeric molecule based on its rank ordering in a flow cytometry-based affinity assay. 1E4 binds to approximately the same location in the extracellular domain of CD20 as does rituximab. Additionally 1E4-based chimeric antibodies co-stain canine B cells in flow cytometric analysis using an anti-canine CD21 antibody. Both 1E4-cIgGB and 1E4-cIgGC were able to significantly deplete B-cell levels in healthy beagle dogs. The in vivo half-life of 1E4-cIgGB in a healthy dog was ~14 days. The antibody 1E4-cIgGB has been selected for further testing and development as an agent for the treatment of canine B-cell lymphoma.10
Other Immunotherapies
1. ImmuneFx™ Cancer Vaccine (Morphogenesis Inc)
ImmuneFx™ is considered a multi-indication cancer vaccine and pre-clinical studies have indicated that ImmuneFx™ acts by providing a priming action for the immune system. The priming antigen is supplied to the patient’s own tumor cells or in vivo in the form of a DNA plasmid. The cellular machinery expresses the antigen on the surface of the tumor cells where it alerts antigen presenting cells to the fact that these cells are now “foreign”. Once this priming action has created an immune response, the antigen presenting cells attack the tumor cells. Preclinical studies have shown that the vaccine can be produced and safely delivered to dogs with naturally occurring lymphoma and a study in dogs with B-cell lymphoma is reported to be underway.11
4. Telomerase vaccine (Takis)
Telomerase reverse transcriptase (TERT) activity is largely confined to tumor tissues and absent in the majority of normal dog tissues making it a valid target for translational cancer immunotherapy. The ability of adenovirus serotype 6 (Ad6) and DNA electroporation (DNA-EP) to induce immune responses against dog TERT (dTERT) in dogs with LSA was evaluated. The vaccine was combined with standard chemotherapy protocol (COP). dTERT-specific immune response was detected in 93% of patient and remained detectable for a prolonged time frame with few associated side effects. The survival time of vaccine/chemo-treated dogs was significantly increased over historic controls of chemo-treated animals.12,13
Summary:
We are making strides and the days of a protocol being a simple “recipe” for all dogs with lymphoma are long gone. We are hopeful that treatment protocols will be based upon the results histologic and immunologic testing, allowing on a basic level, personalized medicine.
References:
1. Thalheim L; Williams LE, Borst LB, et al. J Vet Intern Med. 2013;27:1509-16.
2. Beaver LM, Strottner G, Klein MK. J Am Vet Med Assoc. 2010;237:1052-5.
3. Brodsky EM, Mauldin GN, Lachowicz JL, et al. J Vet Intern Med. 2009;23:578-84.
4. Risbon et al. et al. JVIM 2006;20:1389–1397.
5. Valli VE, Vernau W, de Lorimier LP, et al. Vet Pathol. 2006;43:241-56.
6. Stefanello D, Valenti P, Zini E, et al. J Vet Intern Med 2011;25:90-3.
7. Seelig DM, Avery P, Webb T et al. 2014;28:878–886.
8. Thamm DH, Vail DM, KurzmanID, et al. BMC Veterinary Research 2014;10:30-34.
9. Vail DM, Thamm DH, Reiser H, et al. Clin Cancer Res 2009;15:3503-3510
10. Rue SM, et al. Vet Immunol Immunop 2015; http://dx.doi.org.10.1016/j.vetimm.2015.02.004.
11. http://www.morphogenesis-inc.com/ImmuneFx.html
12. Peruzzi D, et al. Mol Ther 2010;18(8):1559-67.
13. http://www.vetcancertrials.org/studies/vschv-telomerase-vaccine-for-canine-cancer.
Only VETgirl members can leave comments. Sign In or Join VETgirl now!



Interesting article, but still have questions. Recent diagnosis, with phenotyping done, of t-cell lymphoma and we have started CHOP protocol to target one enlarged lymph node (jaw area). I am uncertain if there is better efficacy to be achieved with Tanovea at this point, if we should continue with CHOP protocol. I want more time with my beautiful and loved boxer girl. I will, of course, consult with oncologist, but with the news about Tanovea, I just wonder…
Hi Linda. I saw your comment about your dog with T-cell Lymphoma. I am hoping she made it to remission. My dog was diagnosed in March and we did ChOP too. We are considering Tanovea now as the boy has come out of remission. Please contact me if you have any handy advice. This is hard stuff. Take care, Leslie
Linda and Leslie, I hope your dogs are both still with you. If you would like some onine support, I help moderate a FB group for people whose dogs are undergoing chemo for lymphoma. You can find it here: https://www.facebook.com/groups/LymphomaHeartDogs/
All the best, Ailsa