




July 2026
In this VETgirl online veterinary continuing education blog, Dr. Leah Cohn, PhD, DACVIM, discusses modern advancements in veterinary diabetes mellitus management. Explore key updates, including SGLT2i oral medications for cats, long-acting insulins for dogs and cats, the benefits of user-friendly insulin pens, and continuous interstitial glucose monitoring to improve feline and canine patient care.
What’s New in Diabetes Management
Dr. Leah Cohn, PhD, DACVIM, Professor, University of Missouri, College of Veterinary Medicine
Insulin has now been used to treat diabetes mellitus (DM) in humans for just over a century, but in the last two decades, there have been tremendous changes in treatment and monitoring. Only very recently has veterinary medicine begun to take advantage of some of the same improvements in care for human diabetics. This talk will focus on a few such improvements, including the use of oral SGLT2i drugs for cats, long-acting insulins for dogs and cats, the use of insulin pens, and the use of interstitial glucose monitoring systems.
SGLT2i Drugs
In dogs, DM is almost always due to failure to produce insulin in the pancreatic beta cells and is akin to type I DM in humans; therefore, dogs require insulin therapy. On the other hand, in many cats (up to 80%), DM is the result of insulin resistance, akin to type II DM in humans, wherein the cat still produces its own insulin. In such cats, the initial requirement for more insulin than is available leads to hyperglycemia that then results in beta-cell dysfunction. With time, beta cell loss occurs with a lack of insulin production as well as the original resistance to insulin.
Glucose is freely filtered at the glomerulus, and in healthy animals, the sodium-glucose cotransporter (SGLT) actively reabsorbs the filtered glucose in the tubules. The flozin class of drugs inhibits the SGLT2 that is responsible for 97% of renal glucose resorption, allowing excess glucose to be eliminated from the body and returning the animal to a more euglycemic state while avoiding hypoglycemia. SGLT2i drugs do NOT serve the same purpose as insulin, and animals that lack insulin production require insulin administration for carbohydrate, fat, and protein metabolism. That is why flozin drugs alone will never be an acceptable treatment for dogs, and they are not an acceptable treatment for all cats. Nevertheless, the large majority of cats that still make insulin themselves are often good candidates for chronic management with flozins instead of inulin.
Blood glucose monitor (Image courtesy of Amanda M. Shelby)
Bexagliflozin (tablet) and velagliflozin (liquid) are the approved SGLT2i drugs for treating cats with DM. Given the right choice of patient, these drugs are effective in 80 to 90% of treated cats. Cats that do not make their own insulin are not candidates for flozin treatment. Since there is no easy way to tell which cats do or do not still make insulin, we use comorbid conditions, ketosis, or illness associated with DM as a surrogate marker. Thus, “healthy” diabetic cats are good candidates, while cats who have ketosis or serious comorbid conditions/illnesses are not candidates.
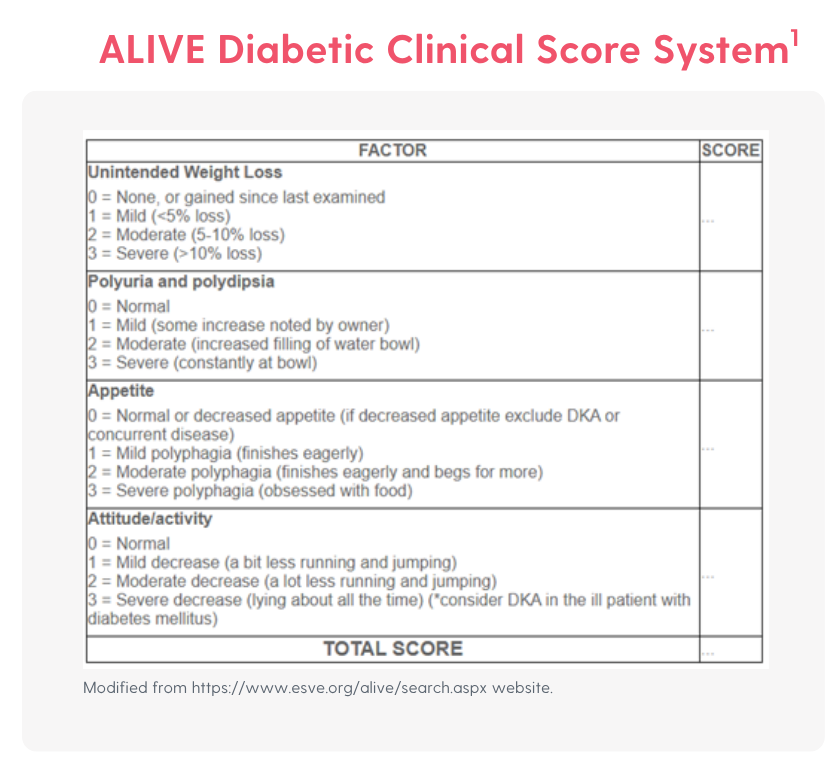
Initial SGLT2i treatment must be monitored by attentive client observation (appetite, attitude, illness signs, as well as improvement in clinical signs attributed to DM) and routine monitoring for ketones. The ALIVE Diabetic Clinical Score System can be useful in evaluating these cats (table). Specific monitoring recommendations vary with drug but generally include measuring ketones at day 3 and weeks 1, 2, 4, and 12 after starting the flozin. Blood ketones (e.g., Abbot Precision Xtra) are more sensitive than urine dipsticks that do not measure the major ketone, b-hydroxybutyrate (BHB). At these same visits, body weight is also assessed. An initial baseline fructosamine can be compared to fructosamine at weeks 4 and 12 to assess glycemic control instead of performing glucose curves. If ketosis is to develop in cats treated with SGLT2i drugs instead of insulin, it usually occurs in the first few weeks after treatment is begun. Illness or more than minimal ketone development (e.g., BHB >4 mmol/L) would be indications to switch the cat to insulin. After the initial 3-month treatment period, monitoring of cats that are doing well on the flozin can be largely clinical with measurement of ketones and fructosamine 2 or 3 times per year. Thus far, there is no indication that glucose curves are required in flozin treated cats.
The most common adverse reactions to these drugs are GI signs, and those are usually self-limiting. The most serious adverse event is euglycemic ketoacidosis. Any cat that becomes ill after starting treatment, at any time, should be tested for ketones, as they may be ketotic despite normal blood glucose. In such cases, supportive care (eg, fluids, electrolytes, nutrition) and insulin therapy (with additional dextrose since the blood glucose will be normal) are mandatory. Hypoglycemia can occur if insulin is administered, but it is quite unlikely in cats treated with SGLT2i alone, a real advantage to the use of flozin drugs. Urinary tract infections or subclinical bacteriuria have also been reported in SGLT2i-treated cats, but at a rate similar to that of insulin-treated cats. Mild hypercalcemia has been reported in a few flozin treated cats, and it might be worth checking blood calcium at the 12-week visit.
Flozin drugs have recently gained tremendous importance in protecting the kidneys and cardiovascular system in people with or without diabetes. It may turn out that these drugs offer advantages to cats or even dogs with renal or cardiac disease. Further, with more investigation, there may be future roles for a combination of treatment with insulin and flozin drugs in diabetics with persistent severe hyperglycemia despite adjusted insulin therapy, but more study is needed.
Long-acting Insulins
In humans, treatment of insulin-dependent (type I) DM now often relies on the use of long-acting basal insulins (aka, peakless insulin) with intermittent bolus administration of immediate short-acting insulin on an “as needed” basis guided by both glucose monitoring, diet, and activity. These “basal-bolus protocols” have led to tremendous improvement in glucose regulation in people with type I DM. For the most part, veterinary insulin administration has lagged behind and still relies on twice daily use of intermediate or long-acting insulins given at the time of feeding to create a nadir in glucose (with risk of hypoglycemia) that then rises until the time of the next injection. Typical veterinary insulins that act in this way include Vetsulin, NPH, PZI, and glargine U100.
Interest and research have grown in recent years regarding the use of insulin types that are considered basal in humans (e.g., glargine U300 [Toujeo®], degludec [Tresiba®]) and are long-acting in animals. We still do not have true basal insulins in our species of interest. However, longer-acting insulins may offer the chance for once-daily insulin with flexibility to pet owners and do not require close timing for feeding or even for insulin administration. These insulin preparations may have less risk of hypoglycemic nadir events and demonstrate less intra- and inter-dose variability. For a brief period, detemir insulin was used as a long-acting (sometimes once daily) insulin in pets, but it is no longer available. On occasion, PZI can be used once daily in cats but not in dogs. Insulin glargine U300 has differing pharmacokinetics from the “usual” glargine U100 that most veterinarians are quite familiar with (Lantus, Semglee, Basaglar). The dense U300 concentration forms a depot with slow insulin release. In cats, glargine U300 has a duration of ~16 hours and can sometimes, but not always, be used once daily in this species. Glargine U300 can also sometimes be used once daily in dogs.
Insulin degludec (U100 and U200 formulations) also forms a depot with protein binding and delayed, slow release in humans and dogs, but with kinetics closer to those of intermediate-acting insulin in cats (i.e., requires BID administration in cats). Degludec has been used quite successfully once daily in 28/33 treated dogs in a small study. Determination of the efficacy of once daily dosing is best achieved via continuous glucose monitoring that allows a rapid adjustment of dose based on response to insulin.
Additionally, there is promising work on the use of ultra-long-acting insulin in dogs and cats. Such insulin is fused with the Fc fragment of immunoglobulins. This fusion protein binds to the host neonatal Fc receptor (FcRn), which leads to recycling of the insulin intracellularly to extend its half-life. This insulin can be injected once per week and has worked well in small studies, but larger clinical trials have not yet been published. An ultra-long-acting (1 week) insulin for humans, insulin icodec, does not have the duration of action in dogs or cats that it does in humans.
Insulin Pens
Veterinarians are comfortable with the use of needles and syringes for insulin administration, but often less so with insulin pens. There is no reason to be afraid of pens! All of the newer, longer-acting insulins are available in pen form, and some are available ONLY in pen form. The insulins we are all familiar with can also be had in pen form, or for use in pens designed to work with insulin from a bottle (Vetsulin can be used in VetPen® by Merck Animal Health). Insulin pens offer numerous advantages, beginning with improved accuracy. The lower the dose of insulin used, the more accurate a pen is compared to a needle and syringe. Studies document that for doses <5 U, there is a 20% dosing error in 50% of administrations. That means for most cats and many dogs, our clients are off by 20% half of the time they inject insulin! Most insulin pens dose in 1 unit increments, but the VetPen® offers 0.5 unit increments for fine adjustment. In addition to the advantage of more accurate dosing, pens offer advantages to people with issues related to manual dexterity or eyesight as well, and are often a better choice for elderly clients.

Insulin pens either contain prefilled cartridges (the long-acting insulins made for people) or fillable cartridges (VetPen). Vetsulin is a suspension (as are PZI and NPH) that must be shaken before use, be that from a bottle or a pen. The long-acting insulin types (e.g., degludec, glargine) are solutions rather than suspensions and do not need to be shaken, rolled, or otherwise mixed.

There are some differences in how pens are used for the treatment of humans vs. pets, as outlined below. For those of you who have not yet used insulin pens, they still require a new needle with each use. The needles look and are packaged differently from the needles you are likely used to using, but they are readily available for purchase. The client can just eject the needle after use into an empty milk jug or the like for disposal. Below are several statements regarding the use of insulin pens. Not all of these statements are yet supported by science, but they are supported by experience.
- People are instructed to “prime” (i.e, “air shot”) by shooting out 3-5 U of insulin into the air before giving themselves an injection. This would be a huge waste of the drug for animals, and it has been adequate to do an “air shot” with a new pen once, then not again on future uses.
- Without priming, air bubbles can occur. Tilting the pen during injection so that the plunger is higher than the needle tip helps draw any air bubbles away from the needle. Pinch up the animal’s skin over the dorsum and stick the pen straight down into the pinched tissue to deploy.
- Store the pen without a needle attached to minimize the risk of air bubbles entering the cartridge. You can look at the insulin periodically to look for changes in clarity or large air bubbles.
- People are told to keep the pen at room temperature, but they are also told to discard the insulin after a set time (typically 28 to 42 days). For people, this allows for the pen to be carried around as in a purse, and a person would use about the entire volume of the pen by the time the “time is up”. For animals, even on what we might consider a high dose of insulin, there is likely to be a lot of insulin left in the pen at the “time up” point. For that reason, I suggest keeping the insulin pen in the refrigerator even if labeled for room temperature storage to help discourage bacterial growth, but keep using the pen. Very likely, it can be used until it is empty, but certainly for up to 6 months. Refrigeration is not often a problem for pet owners, as they don’t often take their dog out to lunch or dinner away from home.
- The disposable needle for pens for pets should not be overly thin to allow penetration of skin; typically, 29-gauge and 0.5-inch is an appropriate size for pets, while the smaller needles work fine on human skin but are not so great for furred dogs and cats.
- In people, the pen is generally kept under the skin to a count of 5 or 10 to make sure the full dose is deployed. With the smaller doses used in pets, this count does not seem to be necessary. Just push the plunger, wait a second, and pull the needle/pen out.
Interstitial Glucose Monitoring
Wearable Continuous Glucose Monitoring (CGM) systems have changed the treatment of DM in humans and animals. The most frequently used system in pets is the FreeStyle Libre (Abbott Labs), although the company does not support its use in animals. Systems specifically for use in animals are in development but not yet available, while other systems for people have been used on occasion in pets. These systems monitor interstitial rather than blood glucose for up to 14 days at a time; interstitial glucose lags behind blood glucose by ~15 minutes. The term “flash” glucose monitoring system simply means that glucose readings are displayed when the sensor is scanned by a reader or smartphone app.

CGM (Image courtesy of Amanda M. Shelby)
The client can view glucose in real time or later via graphs, and the same graphs are available to the veterinarian. Using this system, technician visits are often adequate for placement and removal of the device, but the time required for the veterinarian’s input must be considered. Moment-by-moment knowledge of glucose can be a good thing or a bad thing, depending on the client. The use of CGM systems allows detection of hypoglycemic events that are not clinical and may worry clients needlessly. The systems do not record values above 350 mg/dL, although values up to 500 can be read in real time. The system does allow determination of the proportion of time spent in or above the target range, as well as nadir (though it may be inaccurate at low readings), which can more confidently allow rapid dose adjustment, considering at least a few days of data.
Other Therapies
Other insulin delivery methods are in use in humans but not yet in pets. These include aerosolized insulin (Afrezza®), oral insulin (in trials), infusion pumps and patches, smart insulin systems that allow release of insulin only on an as-needed basis (tied to CGM or glucose-responsive matrix/element), and beta cell replacement therapies (NEJM, DOI: 10.1056/NEJMe2507578)
Reference:
- Niessen SJM, Bjornvad C, Church DB, et al. Agreeing Language in Veterinary Endocrinology (ALIVE): Diabetes mellitus – a modified Delphi-method-based system to create consensus disease definitions. Vet J. 2022;289:105910. doi: 10.1016/j.tvjl.2022.105910. Epub 2022.
Suggested Readings
Behrend EN, Ward CR, Chukwu V, et al. Velagliflozin, a once-daily, liquid, oral SGLT2 inhibitor, is effective as a stand-alone therapy for feline diabetes mellitus: the SENSATION study. J Am Vet Med Assoc. 2024;262(10):1343-1353. doi: 10.2460/javma.24.03.0174.
Cook AK, Behrend E. SGLT2 inhibitor use in the management of feline diabetes mellitus. J Vet Pharmacol Ther. 2025;48 Suppl 1(Suppl 1):19-30. doi: 10.1111/jvp.13466. Epub 2024.
Del Baldo F, Fracassi F. Continuous Glucose Monitoring in Dogs and Cats: Application of New Technology to an Old Problem. Vet Clin North Am Small Anim Pract. 2023;53(3):591-613. doi: 10.1016/j.cvsm.2023.01.008. Epub 2023.
Fleeman L, Gilor C. Insulin Therapy in Small Animals, Part 1: General Principles. Vet Clin North Am Small Anim Pract. 2023;53(3):615-633. doi: 10.1016/j.cvsm.2023.02.002. Epub 2023.
Fleeman L, Gilor C. Insulin Therapy in Small Animals, Part 2: Cats. Vet Clin North Am Small Anim Pract. 2023;53(3):635-644. doi: 10.1016/j.cvsm.2023.02.004. Epub 2023.
Fleeman L, Gilor C. Insulin Therapy in Small Animals, Part 3: Dogs. Vet Clin North Am Small Anim Pract. 2023;53(3):645-656. doi: 10.1016/j.cvsm.2023.02.003. Epub 2023.
Gilor C, Fleeman LM. One hundred years of insulin: Is it time for smart? J Small Anim Pract. 2022;63(9):645-660. doi: 10.1111/jsap.13507. Epub 2022.
Gilor C, Hulsebosch SE, Pires J, et al. An ultra-long-acting recombinant insulin for the treatment of diabetes mellitus in cats. J Vet Intern Med. 2021;35(5):2123-2130. doi: 10.1111/jvim.16150. Epub 2021. Erratum in: J Vet Intern Med. 2023;37(3):1286. doi: 10.1111/jvim.16706.
Hulsebosch SE, Pires J, Bannasch MJ, et al. Ultra-long-acting recombinant insulin for the treatment of diabetes mellitus in dogs. J Vet Intern Med. 2022;36(4):1211-1219. doi: 10.1111/jvim.16449. Epub 2022. Erratum in: J Vet Intern Med. 2023;37(2):782. doi: 10.1111/jvim.16667.
Linari G, Fleeman L, Gilor C, et al. Insulin glargine 300 U/ml for the treatment of feline diabetes mellitus. J Feline Med Surg. 2022;24(2):168-176. doi: 10.1177/1098612X211013018. Epub 2021.
Miller M, Pires J, Crakes K, et al. Day-to-day variability of porcine lente, insulin glargine 300 U/mL and insulin degludec in diabetic dogs. J Vet Intern Med. 2021;35(5):2131-2139. doi: 10.1111/jvim.16178. Epub 2021.
Mott J, Gal A, Tardo AM, et al. Insulin degludec 100 U/mL for treatment of spontaneous diabetes mellitus in dogs. J Vet Intern Med. 2025;39(1):e17303. doi: 10.1111/jvim.17303.
Porter LT, Mott J, Gilor C. Improving owner compliance with therapy of canine and feline diabetes: the American perspective. Companion Animal. 2025;30(4):2-9.
Reinhart JM, Graves TK. The Future of Diabetes Therapies: New Insulins and Insulin Delivery Systems, Glucagon-Like Peptide 1 Analogs, Sodium-Glucose Cotransporter Type 2 Inhibitors, and Beta Cell Replacement Therapy. Vet Clin North Am Small Anim Pract. 2023;53(3):675-690. doi: 10.1016/j.cvsm.2023.01.003. Epub 2023.
Taylor S, Cannon M, Church D, et al. iCatCare 2025 consensus guidelines on the diagnosis and management of diabetes mellitus in cats. J Feline Med Surg. 2025;27(11):1098612X251399103. doi: 10.1177/1098612X251399103. Epub 2025.




Only VETgirl members can leave comments. Sign In or Join VETgirl now!