




June 2025
In this VETgirl online veterinary continuing education blog, Amanda M. Shelby, RVT, VTS (Anesthesia & Analgesia) explains how to recognize the occurrence of rebreathing of carbon dioxide (CO2) in intubated patients, the causes for rebreathing of CO2 and its consequences. Without prompt recognition and treatment, the veterinary patient can quickly deteriorate with some outcomes being life-threatening!
Rebreathing Carbon Dioxide (CO2) in Veterinary Medicine: Identifying Causes
By Amanda M. Shelby, RVT, VTS (Anesthesia & Analgesia), VETgirl Senior CE Specialist
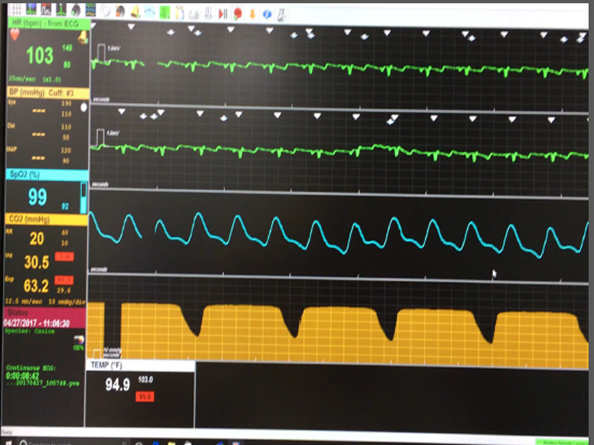
Hopefully in the video above, you recognize quickly that this patient has significant rebreathing of CO2 occurring! But don’t worry, after reading this blog, you’ll be able to recognize rebreathing of CO2 and understand the common causes related to patient anesthesia breathing systems.
A Review of the Fundamentals
Capnography measures CO2, the by-product of cellular metabolism, as it is removed from the body via the respiratory system during exhalation. The measurement of expired CO2 with capnography allows for a non-invasive, real-time assessment of ventilation and circulation. Use of capnography in intubated, anesthetized, patients have demonstrated decreased morbidity and mortality in human and veterinary species.(2-5) For these reasons, capnography is a monitoring favorite by anesthetists and others. In fact, it’s my go-to (and favorite) monitoring device as a veterinary anesthetist! In most mammalian species, normal end-tidal CO2 (EtCO2) is 35-45 mmHg. Normal fraction of inspired CO2 (FiCO2) is 0 mmHg.
Looking at Figure 2, expiration is from A to C, represented by the red line and inspiration is represented as the yellow line. The presence of CO2 during the inspiratory phase in intubated patients indicates inappropriate ventilation and/or a mechanical failure of anesthesia equipment. By understanding causes of rebreathing CO2 as they relate to the breathing circuit in use allows the anesthetist to quickly resolve the issue.

Figure 2. A capnograph. Inspiration is represented by the yellow line and the expiratory phase is represented by the red line. (Image courtesy of Amanda M. Shelby)
Consequences of Hypercapnia (e.g., elevated EtCO2)
But first, before we identify the causes for increased FiCO2 during anesthesia, we should review the consequence of hypercapnia (e.g., elevated EtCO2). CO2 is a weak acid; increases in the partial pressure of CO2 in the blood (PaCO2) causes a decrease in pH which could result in a respiratory acidosis. Elevations in CO2 also can do the following:
- Influence vascular tone (resulting in vasodilation)
- Potentially increase intercranial pressure (ICP) through an increase in cerebral perfusion pressure (CPP)
- Decrease myocardial contractility, further perpetuating hypotension,
- When extremely excessive can result in death.
However, monitoring ventilation with capnography increases awareness of ETCO2 and FiCO2 values allowing the anesthetist to assist or control ventilation where necessary. In the absence of ventilation to perfusion (V/Q) mismatching, EtCO2 should reflect PaCO2, albeit at a slightly lower value.
Common Causes for Elevated FiCO2
A normal inspiratory to expiratory ratio (I:E) is 1:2 (e.g., one second of inspiration in, two seconds of expiration). Regardless of patient breathing system, an inappropriate inspiratory to expiratory ratio (I:E) like that experienced when a patient pants (i.e., I:E of 1:1) can result in rebreathing of CO2. Common causes for an inappropriate I:E ratio of 1:1 could be iatrogenic (i.e. caused by the anesthetist through inappropriate ventilator settings), a patient that becomes light under anesthesia resulting in tachypnea (i.e. panting) or other causes of tachypnea (e.g. hypoxemia). More commonly causes of rebreathing of CO2 involve failure of a part of the anesthetic machine or patient breathing circuit. Figure 3 breaks down general causes unique to the categorical types of patient breathing systems used in veterinary medicine.
 Understanding the impact of fresh gas flow (FGF) rates on determining the degree of rebreathing that can occur in the patient breathing circuit is a foundational step to performing anesthesia. Less rebreathing of expired gases occurs with the use of higher FGF rates. In veterinary medicine, FGF rates are primarily 100% oxygen with a small percentage of halogenated gases (i.e. inhalant anesthetics). Perhaps inappropriately, breathing circuits are commonly referred to as rebreathing, more appropriately termed circle systems and non-breathing systems, more appropriately called Mapleson circuits. When circle systems use oxygen flow rates of 10-30 mL/kg/min, rebreathing of expired gases can occur.(1) Benefits of using a circle (or rebreathing) patient breathing circuit include conservation of resources such as patient body heat, humidity, inhalant use, minimize environmental impact of waste anesthetic gases (WAGs) and oxygen use. Unlike circle systems, Mapleson (or non-rebreathing) circuits are designed to only be used with high oxygen flow rates (i.e. 200 mL/kg/min or greater).(1) Circle systems have unidirectional valves that designate inspiration and expiration hosing as well as CO2 absorption granules that remove CO2 from expired gases before a portion is recycled into the inspiratory limp of the circle system. When a Mapleson system is selected, the absence of unidirectional valves and CO2 absorber makes this patient breathing system dependent on fresh gas flow rate to prevent rebreathing of CO2, in other words, unidirectional flow of gases in the circuit hosing.
Understanding the impact of fresh gas flow (FGF) rates on determining the degree of rebreathing that can occur in the patient breathing circuit is a foundational step to performing anesthesia. Less rebreathing of expired gases occurs with the use of higher FGF rates. In veterinary medicine, FGF rates are primarily 100% oxygen with a small percentage of halogenated gases (i.e. inhalant anesthetics). Perhaps inappropriately, breathing circuits are commonly referred to as rebreathing, more appropriately termed circle systems and non-breathing systems, more appropriately called Mapleson circuits. When circle systems use oxygen flow rates of 10-30 mL/kg/min, rebreathing of expired gases can occur.(1) Benefits of using a circle (or rebreathing) patient breathing circuit include conservation of resources such as patient body heat, humidity, inhalant use, minimize environmental impact of waste anesthetic gases (WAGs) and oxygen use. Unlike circle systems, Mapleson (or non-rebreathing) circuits are designed to only be used with high oxygen flow rates (i.e. 200 mL/kg/min or greater).(1) Circle systems have unidirectional valves that designate inspiration and expiration hosing as well as CO2 absorption granules that remove CO2 from expired gases before a portion is recycled into the inspiratory limp of the circle system. When a Mapleson system is selected, the absence of unidirectional valves and CO2 absorber makes this patient breathing system dependent on fresh gas flow rate to prevent rebreathing of CO2, in other words, unidirectional flow of gases in the circuit hosing.
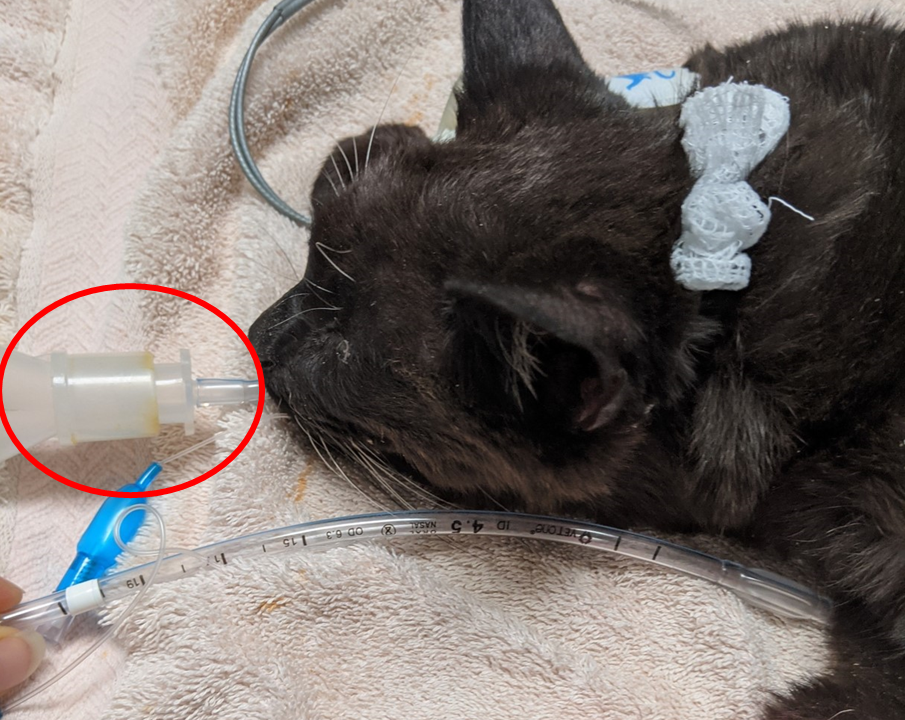
Figure 4. Area within the red circle is dead space, while not excessive in this patient could become excessive with large capnograph adaptors, excessively long endotracheal tubes and other breathing circuit adaptors (e.g. elbows). (Image courtesy of Amanda M. Shelby)
Regardless of which patient breathing circuit in use, when patients have inappropriate I:E ratios less than 1:2, excessive dead space which is any space inspiratory and expiratory gases can mix (See Figure 4 as an example) or a leak between co-axial tubes. Co-axial tubes are breathing circuits designed with the inspiratory tubing inside the expiratory tubing (e.g. modified Bain circuit designed to be used with non-rebreathing FGF rates or the F-circuit circle system designed to be used as a rebreathing circuit) (See Figure 5 and 6). A thorough understanding of the patient breathing circuits’ leading causes for an increase in FiCO2 assists with rapid identification of the cause.

Figure 5. Mapleson patient breathing circuits designed to be used with non-rebreathing FGF rates. Mapleson circuit (left); Modified Bain circuit (right). (Image courtesy of Amanda M. Shelby)

Figure 6. Circle systems hanging. Pediatric 15 mm ID tubing circle system (left); Traditional 22 mm ID tubing circle system (right). (Image courtesy of Amanda M. Shelby)
So, how do you prevent rebreathing of CO2 in your anesthetized patients?
1. Preform leak tests and routine anesthetic equipment check out procedures before each case. Good check out procedures involving routine inspection of all anesthetic equipment, especially breathing circuits with co-axial tubing and performing positive pressure machine checks before use will eliminate many of the common causes for rebreathing of CO2. If using a circle system ensure unidirectional valves are functioning during the positive pressure check out—while filling the circuit with positive pressure the inspiratory valve should open, expiratory valve should remain closed, when the positive pressure is released from the circuit by opening the adjustable pressure limiting (APL or ‘pop-off’ valve), the expiratory valve should open and inspiratory valve should remain closed.
Additionally ensure the CO2 absorption granules are functional. This could include ensuring they crumble when crushed between your fingers. The absence of a color change may not always be an indicator that the CO2 absorption granules are ok to use, especially when a machine is infrequently used.
Become a VETgirl ELITE member and get your learning on! Check out this webinar on how to set up and pressure check your anesthetic machine and select the patient breathing circuit.
2. Calculate appropriate FGF rates based on the patient breathing circuit in use (rebreathing vs. non-rebreathing) specific to the patient’s requirement. See example below:
25 kg dog using a rebreathing circuit FGF of 20 mL/kg/min equals a FGF rate of 500 mL/min.
5 kg cat using a non-rebreathing circuit FGF of 200 mL/kg/min equals a FGF rate of 1000 mL/min or 1 L/min.
*Keep in mind that most anesthetic precision vaporizers require minimum FGF rates of at least 500 mL/min or 0.5 L/min to ensure accurate inhalant output.
3. Reduce dead space. Reduce patient dead space where possible. Use appropriate length endotracheal tubes. Endotracheal tubes can be cut down to size if the portion removed is before the cuff pilot line (see Figure 7). Other methods for reducing dead space include using pediatric tubing for small patients or consider using Mapleson (or non-rebreathing) circuits and pediatric capnograph adaptors.

Figure 7. The red line denotes the lowest point towards the patient end, where this endotracheal tube could be cut to reduce dead space. The cuff pilot line enters to the right of the red line. (Image courtesy of Amanda M. Shelby)
Tips to help you identify the cause for high FiCO2
Lastly, what should you do if your experiencing high FiCO2 and can’t identify the cause? An FiCO2 above 5 mmHg should be concerning. If this continues to elevate and the cause cannot be identified, use of the machine should be discontinued until it can be properly serviced. Since the most often causes are related to unidirectional valves, expired CO2 absorbing granules or the patient breathing circuits, often the causes are easy to identify and resolve. When the issue is related to the patient breathing circuit, regardless of the machine used, rebreathing will continue to occur. If these patient breathing circuits cannot be repaired, it is best to discard and replace them.
For me personally, the hardest source for rebreathing CO2 situations I have experienced has been with leaks in the inner tubes of co-axial circuits (both on Modified Bain circuits and F-circuits) and warped/cracked unidirectional valves. Otherwise, identifying the cause for rebreathing of CO2 is typically straightforward if you following the causes identified in Figure 3.
Conclusion
When in doubt, it is very important that veterinarians and veterinary technicians be aware of how to prevent rebreathing of carbon dioxide (CO2) in intubated veterinary patients. Most of the cause for rebreathing of CO2 can be prevented with similar anesthetic check out procedures that evaluate each component of the anesthetic machine and patient breathing circuit. Being able to prevent, recognize, and treat hypercapnia, we can improve the outcome and safety of anesthesia in our veterinary patients.
Abbreviations:
APL: adjustable pressure limiting or ‘pop-off’ valve
CO2: carbon dioxide
EtCO2: end-tidal CO2
FGF: fresh gas flow
FiCO2: fraction of inspired CO2
I:E: Inspiratory to expiratory ratio
V/Q: ventilation to perfusion
WAGs: waste anesthetic gases
References:
- Shelby AM, McKune CM. Small Animal Anesthesia Techniques. 2 ed. Hoboken, NJ: John Wiley & Sons, Inc.; 2023.
- Henao-Guerrero PN, Hodgson DS, Mason DE. Capnography in veterinary medicine. VAA. 2005;32(4):233-5.
- Langton S, Flaherty D, Pawson P, et al. A serious breathing system fault identified by capnography. VAA. 2010;37(6):581-2.
- Gallagher JJ. Capnography monitoring during procedural sedation and analgesia. AACN Advanced Critical Care. 2018;29(4):405-14.
- Langhan ML, Li FY, Lichtor JL. The impact of capnography monitoring among children and adolescents in the postanesthesia care unit: a randomized controlled trial. Pediatric Anesthesia. 2017;27(4):385-93.
Only VETgirl members can leave comments. Sign In or Join VETgirl now!





Thank you!
This blog is great, I appreciate the focus on limiting dead space and advocating for patient safety during anesthesia while intubated. The reminder of the responsibility support staff have while pressure checking our breathing circuits. Thank you for promoting awareness of the impact of FGF rates on determining the degree of rebreathing that can occur in the patient breathing circuit and the review of the consequences of hypercapnia.
This article came to me at the perfect time! I feel like I’m in a constant battle with our capnograph but it’s also my favourite piece of equipment when it works! This article was amazing and super helpful! Thank you!