





July 2023
By Dr. Garret Pachtinger, VMD, DACVECC, Director of Operations / Co-Founder, VETgirl
Trauma without the Drama: Part 2 with Dr. Garret Pachtinger
If you missed Part I of Dr. Garret Pachtinger’s VETgirl blog “Trauma without the Drama: Part 1,” check it out HERE. Keep reading to learn more about how to approach that trauma small animal patient!
FAST3 Scan – Introduction
FAST3 is an abbreviation for a procedure known as Focused Assessment with Sonography for Triage, Tracking, and Trauma. This is a tool, a diagnostic, that was initially used in human medicine to identify trauma patients with abdominal hemorrhage. The FAST3 protocol has become a common diagnostic tool in the emergency room to scan for free fluid within any body cavity (abdomen, retroperitoneal, pleural, pericardial space).
In the past few years, the abdominal FAST3 protocol has been validated in dogs, reporting a good sensitivity and specificity to detect peritoneal effusion.

FAST3 Scan – Indications
The A-FAST3 scan is a non-invasive, rapid screening tool for abdominal effusion, indicated in patients presenting with trauma, acute abdomen, and other signs of abdominal disease or discomfort.
FAST3 Scan – Benefits
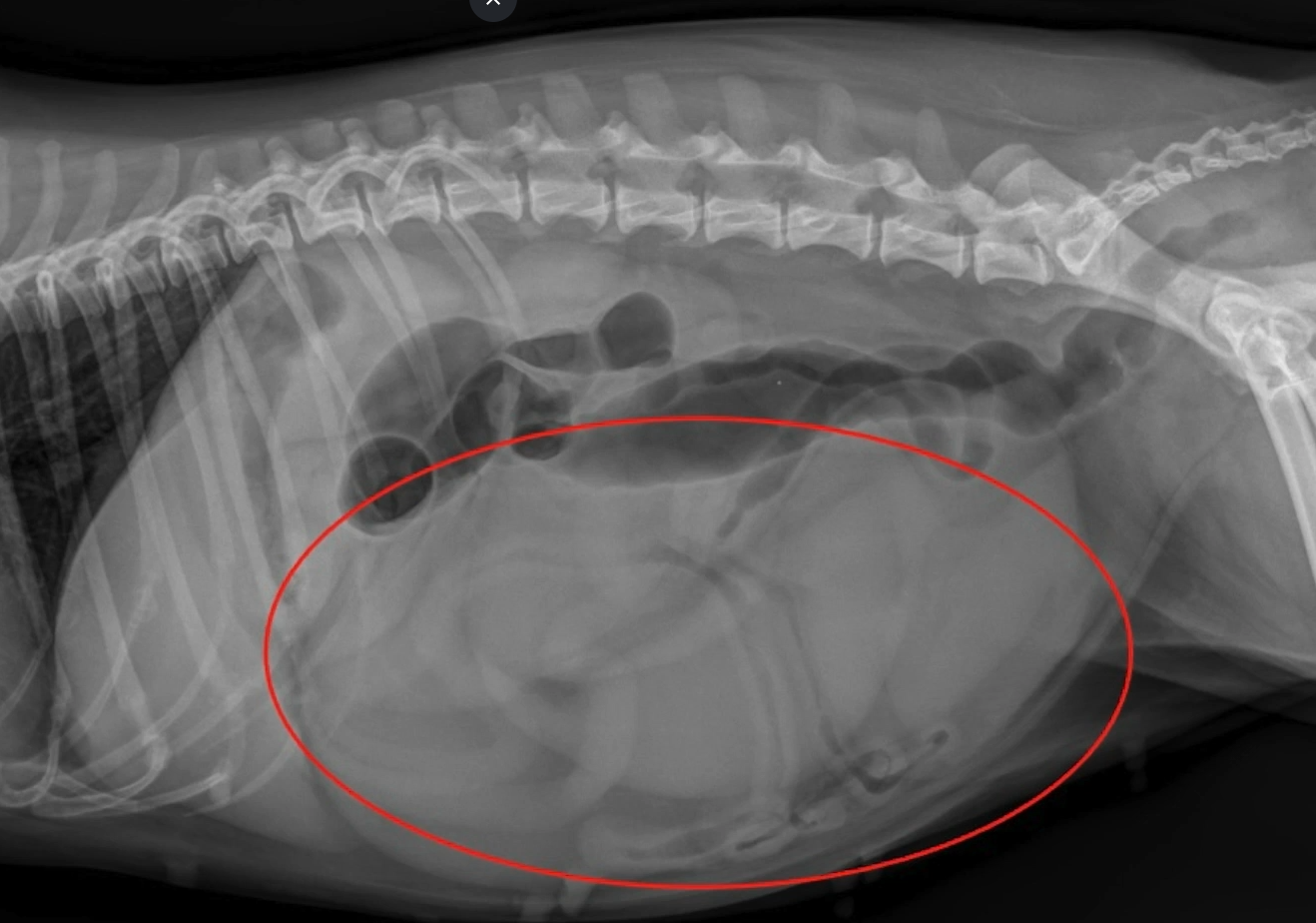
- As compared to radiographs, ultrasonography is more sensitive for detecting effusion.
- FAST3 scans are noninvasive, safe, rapid, and do not require the use of radiation to the patient or veterinary personnel.
- A FAST3 scan can be performed during further patient assessment, catheter placement, and treatment/stabilization.
FAST3 Scan – Technique
- The patient is placed in right lateral recumbency, although if the patient is in distress, they may remain standing or sit in sternal recumbency to facilitate the procedure.
- Theabdomen is evaluated at four distinct sites
- Just caudal to the xiphoid process (diaphragmatic-hepatic view)
- The midline over the urinary bladder (cystocolic view)
- Over the left and right flank regions (splenorenal and hepatorenal views)
- Each site is scanned in two planes at a 90-degree angle to each other.
- Serial exams using the FAST3 protocol may be needed, especially if hypovolemic or in shock to diagnose the presence of effusion
- Serial exams may also be used to monitor the amount of fluid present (i.e. is there ongoing accumulation of fluid)
While a FAST scan is not a complete, thorough ultrasound and it does not replace the utility of diagnostic radiographs, it is an important diagnostic tool for the small animal practitioner and one that the clinician should be comfortable performing.
HEAD TRAUMA:
Severe brain and spinal cord injury are challenging cases to treat in small animal medicine. With trauma severe enough to result in neurologic injury, it is important to recognize the potential for other serious injuries including pneumothorax, pulmonary contusion, traumatic hemoabdomen, uroabdomen, and fractures. As a result, rapid patient assessment and treatment is critical to reduce morbidity and mortality. Many veterinary patients can recover from CNS injuries with rapid patient assessment and treatment.
Pathophysiology of Brain/Spinal Injury
Brain and spinal injury can be divided into primary injury and secondary injury. Primary injury refers to the events that occur immediately at the time of trauma and include direct damage to the parenchyma and vasculature. Examples of primary brain injury include contusions, lacerations, hemorrhage, and vasogenic edema. Secondary injury results from a cascade of physiologic and biochemical events that occur in the subsequent hours to days following the primary injury. Events resulting in secondary brain and spinal injury include depletion of neuronal ATP levels (worsened by hypoxemia or hypovolemia), intracellular accumulation of calcium and sodium ions, oxygen free radical formation, increased cytokine production, elevated extracellular glutamate levels, nitric oxide accumulation, lactic acid accumulation, and activation of other cell-damaging pathways (e.g., kinin, complement, coagulation/fibrinolytic pathways). Primary and secondary injuries to the brain and spinal cord can result in increased morbidity and mortality if not rapidly assessed and treated.
Primary Injury
Head Trauma
Classifications of primary head trauma include concussion, contusion, laceration, intra and extra-axial hematomas, and skull fractures. These are specific and direct abnormalities of the brain parenchyma that occur at the time of the trauma.
Concussion
- Characterized by a brief loss of consciousness
- Not associated with any underlying histopathologic lesions
Contusion
- Bruises of the cerebral parenchyma
- Result from direct trauma of the brain against the skull
- “Coup” lesions – lesions on the side of impact
- “Contrecoup” lesions- lesions on the opposite side of impact due to displacement of the brain during impact
Laceration
- Caused by disruption of the brain parenchyma
- Results in intracranial hemorrhage
- Hemorrhage can result in axial hematomas within the brain parenchyma as well as extra-axial hematomas in the subarachnoid, subdural, and epidural spaces
Spinal Trauma
Examples of primary spinal trauma include vertebral fracture, intervertebral disk herniation, spinal cord contusion, and extra-axial hemorrhage. The severity of the spinal trauma will depend on the severity of the underlying abnormality. With vertebral fractures, the extent of the spinal trauma will depend on the instability and degree of trauma to the actual vertebral process. Similarly, with intervertebral disk herniation may be more damaging with Hansen’s Type I intervertebral disk disease as compared to a type II disc herniation.
Secondary Injury
Secondary injury results from a series of biochemical events following the primary injury including excitotoxicity, ischemia, inflammation, and production of reactive oxygen species, accumulation of intracellular sodium and calcium, nitric oxide accumulation, ATP depletion, and cerebral lactic acidosis. Following the primary trauma, there is an increased release of excitatory neurotransmitters (i.e. glutamate and aspartate). These neurotransmitters activate other receptors, resulting in an increased intracellular sodium and calcium concentration. This increased concentration leads to excessive depolarization and further release of excitatory neurotransmitters. Ultimately, this is a vicious cycle of excitatory stimulation resulting in intracellular damage. Other important cytokines and factors in secondary injury include nitric oxide (NO), Interleukin-1β (IL-1β), Interleukin-6 (IL-6), and Tumor Necrosis Factor α.
Intracranial Pressure (ICP) and Cerebral Perfusion Pressure (CPP)
The skull is a rigid compartment containing the brain, blood and cerebrospinal fluid (CSF). If any of the individual components change, the end result is going to be a change in ICP. Since measurement of intracranial pressure is practically impossible in most clinical settings, it is important to for the clinician to recognize changes in the patient consistent with changes in ICP. Such changes may include pupil changes, ocular position, mentation, breathing pattern (apneustic breathing, or Cheyne-Stokes breathing) or via Cushing’s reflex .
When we evaluate CPP, this is done via the equation:
Cerebral perfusion pressure = Mean Arterial Pressure–Intracranial Pressure (CPP = MAP–ICP)
Ultimately, if ICP rises, MAP must also increase in order to maintain CPP. If there is continued elevation of the ICP without therapy, there will be a decreased CPP and poor perfusion of the pons and medulla. The result is an accumulation of CO2 and sympathetic stimulation to increase systemic blood pressure. Sympathetic stimulation and increased blood pressure triggers a baroreceptor-mediated bradycardia. Hypertension and bradycardia associated with elevated ICP is known as the Cushing’s reflex and suggestive of markedly elevated ICP and impending brain herniation.
Following the triage examination and patient assessment, a more specific neurologic assessment can be made. Neurological assessment should include the patient’s level of consciousness, pupil size and responsiveness, ocular position and eye movements and skeletal motor responses. If there are abnormalities or concerns, this assessment should be repeated every 30–60 minutes. Other examination findings that may indicate possible head trauma include blood within the external ear canals, wounds to the head and / or neck region, episcleral hemorrhage, hyphema, epistaxis, broken teeth, and/or fractures on palpation of the bones of the head.
Neurological Evaluation and the Modified Glasgow Coma Scale
In trying to develop a more objective scale when evaluating the patient with neurological injuries, the Modified Glasgow Coma Score (MGCS) may be a useful indicator of prognosis in the patient with traumatic brain injury (TBI). The MGCS will give not only an initial objective assessment of the neurological status, but this will allow for more objective serial neurologic assessment of the patient with TBI. This scale evaluates three primary areas: level of consciousness, brain stem reflexes, and motor activity/posture. Each category is scored 1-6 with 6 being normal in all categories and 1 being abnormal. The three scores are added and the total provides an objective number for initial and serial patient assessment as well as a 48 h survival prognosis: 3-8 grave, 9-14 guarded, 15-18 good.
Motor activity
- Normal gait, normal spinal reflexes – 6
- Hemiparesis, tetraparesis, or decerebrate activity – 5
- Recumbent, intermittent extensor rigidity – 4
- Recumbent, constant extensor rigidity – 3
- Recumbent, constant extensor rigidity with opisthotonus – 2
- Recumbent, hypotonia of muscles, depressed or absent spinal reflexes – 1
Brain stem reflexes
- Normal pupillary light reflexes and oculocephalic reflexes – 6
- Slow pupillary light reflexes and normal to reduced oculocephalic reflexes – 5
- Bilateral unresponsive meiosis with normal to reduced oculocephalic reflexes – 4
- Pinpoint pupils with reduced to absent oculocephalic reflexes – 3
- Unilateral, unresponsive mydriasis with reduced to absent oculocephalic reflexes – 2
- Bilateral, unresponsive mydriasis with reduced to absent oculocephalic reflexes – 1
Level of consciousness
- Occasional periods of alertness and responsive to environment – 6
- Depression or delirium, capable of responding but response may be inappropriate – 5
- Semi comatose, responsive to visual stimuli – 4
- Semi comatose, responsive to auditory stimuli – 3
- Semi comatose, responsive only to repeated noxious stimuli – 2
- Comatose, unresponsive to repeated noxious stimuli – 1
Important assessments and definitions of the Head/Spinal Trauma Patient
Assessment of level of consciousness.
Alert – Normal behavior, responsive
Depressed – Subdued, awake but uninterested in environment
Delirious – Awake but altered perception, responds inappropriately to stimulus
Stuporous – Remains in sleep state, only aroused by strong stimulus
Comatose – Deep unconsciousness, unable to rouse
Abnormalities of limb posture
Spasticity – Increased muscle tone of the limbs
Opisthotonos – Body posture in which there is rigid or ‘spastic’ extension of the cervical musculature. The head and neck are held in extension with the top of the head directed toward the spine. Opisthotonus is a component of several different postures that can be seen in the recumbent animal.
Decerebrate rigidity – A posture characterized by opisthotonus and rigid extension of all the limbs. Usually caused by severe lesions of the midbrain leading to the loss of descending inhibition from the cerebrum to the portion of the brainstem (medullary reticulospinal tract) responsible for flexion of the limbs. This posture carries a poor to grave prognosis for recovery.
Decerebellate rigidity – A body posture characterized by opisthotonus, thoracic limb extension and pelvic limb flexion. The posture is moist commonly caused by an acute traumatic lesion of the cerebellum. The patient is fully conscious with normal mental awareness, distinguishing it from the decerebrate posture. There is usually a fair to good prognosis for recovery.
Schiff-Sherrington posture – A body posture characterized by thoracic limb extension with pelvic limb paralysis. This posture results from an acute lesion of the thoracic or cranial lumbar spinal cord that interrupts ascending inhibitory impulses originating in the border cells of the lumbar gray matter (primarily L1-5) and terminating on the cells responsible for extension of the thoracic limbs. The posture does not have prognostic significance.
Tetanus – A body posture characterized by severe extensor rigidity of the limbs and other muscles
Abnormalities of trunk posture
Scoliosis – Lateral curvature of the spine
Kyphosis – Dorsal curvature of the spine
Lordosis – Ventral curvature of the spine
Torticollis – Twisting of the neck to one side
Cervical ventroflexion – Ventral positioning of the head with the nose directed toward the ground
Keeping in mind these patients often present in shock, accurate evaluation of mental status should be delayed until hypovolemic shock has been corrected. Common mentation classifications include normal, depressed/obtunded, stuporous, or comatose.
Normal – Alert and appropriately responsive to environment & stimuli
Depressed / obtunded – Quiet / asleep without stimulation, but patient can be roused
Stuporous – Unconscious, but rousable with noxious stimulation
Comatose – Unconscious, unable to rouse with noxious stimuli
Diagnostic Tests
Initial diagnostic tests should include a minimally invasive, global patient assessment. This includes a complete blood count (CBC), serum chemistry panel, and venous blood gas. Jugular veins should be avoided as holding off the vein and phlebotomy may increase ICP. Blood pressure and pulse oximetry are also recommended. In the context of trauma, ultrasonographic evaluation of the chest and abdomen (AFAST/TFAST) are also helpful. Due to the need for sedation or restraint, radiographs are rarely performed on initial patient assessment.
The use of computed tomography (CT) and magnetic resonance imaging (MRI) are more sensitive at detecting intracranial lesions. An MRI is considered to be the best imaging modality for detection of fibrocartilagenous emboli (FCE).
Emergency Treatment of Head and Spinal Trauma
Initial assessment for any trauma patient should address any life-threatening abnormalities. Patients presenting with head or spinal trauma should be assessed for other life threatening abnormalities including shock. Rushing to assess the neurological status without addressing life threatening shock may result in further morbidity and mortality as well as an incorrect neurological diagnosis as patients in shock often exhibit depressed mentation due to the hypotensive state without any true brain injury.
Head Elevation
Stabilization of the head and spine are important priorities with brain and spinal cord injury. WITH head trauma, the patient is placed on a board where their body is supported ultimately resulting in an elevation of the head 15–30 degrees. The goal of this positioning is to encourage cerebral venous drainage, ultimately to decrease intracranial pressure. During this procedure it is important to avoid pressure on the jugular veins or bending of the neck which can decrease venous drainage and increase ICP.

If spinal cord injury is suspected, the patient should be immobilized on a firm, flat surface such as a backboard.
OXYGEN THERAPY
Decreased oxygen delivery is an important contributor to secondary neurological injury. For this reason, oxygen delivery is a priority in treatment of CNS trauma. During initial patient assessment, oxygen can be administered, via ‘flow-by’ or mask. This delivery method allows continued patient assessment and treatment as opposed to an enclosed oxygen cage which will prevent further patient assessment.
FLUID THERAPY
Along with oxygen therapy to address hypoxemia, hypovolemia and shock need to be addressed. Volume resuscitation should be addressed with a goal of a mean arterial blood pressure of 80–100 mm Hg. Fluid therapy options include isotonic crystalloid therapy (LRS, 0.9% NaCl, P-Lyte), hypertonic crystalloid therapy (7.2% NaCl), synthetic colloid therapy (Hetasarch, Vetstarch), or a combination of therapies. Unless there is concurrent complicating disease such as cardiac disease, fluid therapy is important in head trauma patients as hypovolemia compromises cerebral perfusion pressure (CPP). Careful administration of intravenous crystalloid fluids at ¼ – 1/3 of the calculated shock volume of fluids (90 ml/kg in dogs and 60 ml/kg in cats) should be administered with frequent patient reassessment to assess response to therapy. Alternatively, 2-5 ml/kg of a synthetic colloid such as Hetastarch or vetStarch can be administered as an IV bolus.
Hyperosmotic Therapy
If the patient presents obtunded, stuporous, or comatose, hyperosmotic solutions such as mannitol are commonly considered. Mannitol has a rapid onset of action with effects lasting as long as 6 hours. The benefits of mannitol include an immediate plasma expanding effect, reduction in blood viscosity, increased CBF, and increased cerebral oxygen delivery. Treatment should be followed with crystalloids or colloids to maintain intravascular volume. The dose of mannitol 20% is 0.5–1.5 g/kg in dogs and cats. Mannitol is most commonly administered in boluses over 15-20 minutes rather than a CRI to prevent rebound hypotension.
Hypertonic Saline is an alternative hyperosmotic agent and preferred in hypovolemic patients. Hypertonic saline creates an osmotic effect, pulling water out of the CNS and decreasing ICP. The recommended dose for volume expansion is 5-10 ml/kg of 7.5% sodium chloride. The volume expanding effects are immediate but redistribution is rapid, within 15–75 minutes. To create a solution with longer effects, a 1:2 ratio combining 23.4% hypertonic saline with 6% hetastarch can be used, termed “turbostarch.”
Corticosteroids
Corticosteroid use is not currently recommended in the treatment of traumatic brain injury. Although corticosteroids have anti-inflammatory effects, they are associated with several negative issues including hyperglycemia, immunosuppression, delayed wound healing, and gastric ulceration. Hyperglycemia has been shown to be a negative prognostic indicator in humans and dogs with severe head injury.
Regarding spinal trauma, the use of methylprednisolone sodium succinate (MPSS) is currently considered the gold standard of care in spinal trauma (30 mg/kg IV once, then 15 mg/kg IV 2 and 4–6 hours later). The time frame for reported benefits in human patients is administering the MPSS within 8 hours of the traumatic event. After this time frame, there has been no documented benefit of steroid use in helping improve prognosis for return to function.
Summary
Traumatic brain injury and spinal trauma are common presentations to the small animal clinician. Initial assessment must be a global patient assessment, with careful evaluation of the ABCDs of triage medicine. Rapid and direct patient assessment are best made to reduce morbidity and mortality in the polytrauma patient.
For References, please see Part 1 of Trauma without the Drauma



Only VETgirl members can leave comments. Sign In or Join VETgirl now!