





July 2023
By Dr. Garret Pachtinger, VMD, DACVECC, Director of Operations / Co-Founder, VETgirl
Trauma without the Drama: Part 1 with Dr. Garret Pachtinger
In Part 1 of a two-part VETgirl online veterinary continuing education blog, Dr. Garret Pachtinger, DACVECC, provides a case-based, practical approach to trauma treatment. Don’t forget to tune into PART 2 HERE in a few weeks to learn more!
Trauma without the Drama: Part 1 with Dr. Garret Pachtinger
Trauma is one of the most common emergencies seen in the busy emergency room. Examples of common veterinary trauma presentations include motor vehicle accidents (i.e. hit by car) interaction with other animals, interaction with humans, fall from heights, and penetrating trauma such as gunshot wounds, knife wounds, and impalement by sticks. Trauma may affect only one body system, or it may affect multiple organ systems. For this reason, the initial approach to the trauma patient must be rapid, thorough, and detailed to decrease further morbidity and mortality.
The initial triage evaluation should be rapid, developing a problem list outlining life-threatening conditions. The goals of the initial triage examination are to:
- Assess / evaluate the ABCD’s of triage medicine:
-
- Airway: Does the patient have a patent airway? Upper airway or lower airway abnormalities?
- Breathing: Does the patient have an abnormal breathing pattern? Is the patient dyspneic? Is there a rapid, shallow breathing pattern? Is there a slow, labored breathing pattern? Is there increased stertor or stridor?
- Circulation: Is there an abnormal heart rate? Are the mucous membranes an abnormal color with evidence of internal or external hemorrhage? Are the pulses weak? Are the extremities cold?
- Disability: Is there evidence of head trauma or other neurological injury?
- Exsanguination: Is there evidence of (life threatening) bleeding

-

- Specifically, regarding thoracic trauma, the goal is to rapidly determine if there are respiratory abnormalities. If present, the goal is to localize the cause for respiratory distress to best provide treatment:
- Inspiratory wheezes: associated with narrowing of the upper airways by inflammation, hemorrhage, mucosal edema, or mucus.
- Expiratory wheezes: associated with narrowing of the lower airways by inflammation, hemorrhage, mucosal edema, or mucus.
- Crackles: fluid present within the lower airways / alveoli (e.g. edema, hemorrhage)
- Stridor or stertor: indicates an upper airway respiratory abnormality
- Short / shallow pattern: may indicate pleural space disease such as pneumothorax, pleural effusion, or diaphragmatic hernia
- Paradoxical breathing: recognized by a lack of synchronous movement of the chest and abdominal walls.
Initial therapy chosen will be based on the degree and location of injury. Common therapies include oxygen supplementation, intravenous fluid therapy, and analgesia. Procedures such as a thoracocentesis may also be required, which can be both diagnostic and therapeutic.
Oxygen supplementation is one of the mainstays of therapy for a patient with respiratory difficulty. Initially, oxygen is often provided by facemask or flow-by to permit the clinician to perform the initial assessment. While oxygen cages may allow a higher percentage of oxygen to be delivered, it is difficult to assess the patient once in the closed oxygen cage, and therefore placement into the oxygen cage is often delayed until after initial assessment has been performed.
Oxygen Supplementation Techniques.
| Supplementation technique | Required flow rate | Maximum inspired oxygen concentration achieved |
| Flow-by | 3-15 l/min | 40% |
| Oxygen cage | 15 l/min | 45-60% |
| Oxygen hood (unsealed bag) | 5-15 l/min | 85-95% |
| Oxygen collar | 1 l/10 kg bodyweight/min | <80% |
| Nasal cannula | 50-100 ml/kg/min | 40% |
| Nasal catheters | 50-100 ml/kg/min | 40-50% |
| Nasopharyngeal catheter | 50-100 ml/kg/min | 60-70% |
| Nasotracheal catheter | 25-50 ml/kg/min | 80-90% |
Intravenous access for fluid therapy and drug administration is also important. Initially, intravenous access is preferred via the use of by peripheral veins, notably the cephalic or saphenous veins. Other sites such as the jugular vein, while available, are not preferred as placement is not only more technically challenging but requires increased restraint which can be distressing to the dyspneic patient. Moreover, the use of the jugular vein should be avoided if there is a concern for head trauma and increased intracranial pressure. If patient stability allows, when placing the catheter, it is advised to pull blood for anticipated testing including a minimum database (packed cell volume (PCV), total protein (TP), Azostick / dipstick BUN, and blood glucose concentration). A complete blood count, chemistry panel, and coagulation panel can also be drawn at that time if patient stability allows.
Once intravenous access is obtained, fluid therapy for resuscitation can be initiated. The goal of fluid resuscitation is to restore tissue perfusion and oxygenation. The type, volume, and rate of fluid administration are determined based on the patient assessment and underlying injuries. The two most common fluid choices for the resuscitation phase are isotonic crystalloids and synthetic colloids. Examples of isotonic crystalloid replacement fluids are 0.9% saline, lactated Ringer’s solution, Normosol-R or Plasmalyte-A. Typically, smaller doses of fluids are administered (10-30ml/kg in the dog, 5-10ml/kg in the cat) with frequent re-assessment rather than large volumes at once with the risk of worsening respiratory distress. Colloids are larger molecular weight fluids considered intravascular volume expanders. Examples of synthetic colloids include Hetastarch and Vetstarch. Typically, smaller doses of fluids are administered (2-5ml/kg in the dog, 1-3ml/kg in the cat) with frequent re-assessment rather than large volumes at once with the risk of worsening respiratory distress. Once initial evaluation, treatment, and stabilization have started, the clinician can further evaluate the patient with a more thorough general examination to assess other complications of thoracic trauma.
Airway Trauma
Trauma to the major airways may be seen with penetrating wounds or blunt trauma to the neck and chest. Clinical signs of upper airway trauma include abnormal upper airway noise on inspiration and expiration. Respiratory changes may result from traumatic inflammation, edema, hemorrhage, or even tracheal rupture or avulsion.
Subcutaneous emphysema may also be noted on examination, prompting a thorough airway integrity assessment. Pneumomediastinum and pneumothorax are more severe complications of airway trauma. While subcutaneous emphysema and pneumothorax may be easily found on examination alone, the diagnosis of pneumomediastinum is made radiographically by increased contrast with the mediastinal structures resulting in a clear visualization of the thoracic vena cava, aorta and esophagus.
Pneumothorax
Pneumothorax is defined as the abnormal accumulation of air in the pleural space. Air accumulation is most commonly bilateral but unilateral pneumothorax can occur. It is the most common complication of blunt trauma to the chest. Studies have shown that animals hit by car with fractures had evidence of pneumothorax 47.1% of the time. Furthermore, 36% of dogs and 63% of cats that fell from high rises that had evidence of pneumothorax on examination. Pneumothorax can be further classified as closed, open, and tension pneumothorax.
- Closed pneumothorax is seen following trauma due increased intra-thoracic pressure against a closed glottis causing rupture of alveoli or small airways, laceration of lung by fractured rib, iatrogenic, and airway or esophageal rupture causing pneumomediastinum which has progressed to pneumothorax.
- Open pneumothorax may result from gunshots, dog bites, knife wounds, and stick impalement.
- Tension pneumothorax is the third type, resulting when an air leak acts as one-way valve increasing intrathoracic pressure, compressing the lungs and decreasing venous return to the heart.
The astute clinician often makes the diagnosis of a pneumothorax based on history and examination alone. Common examination abnormalities include an increased respiratory rate and effort characterized by a short and shallow breathing pattern, dull lung sounds dorsally, and muffled heart sounds. Less specific examination abnormalities may include pale or cyanotic mucous membranes, poor pulses, and an abnormal posture with the head and neck extended and elbows abducted. While useful in the diagnosis of a pneumothorax, thoracic radiographs risk increased stress on the compromised patient. Radiographic signs of pneumothorax include elevation of the cardiac silhouette from the sternum, collapse of the lung lobes, and absence of vascular markings out to the periphery of the thorax.
Recently, the use of ultrasound has been documented for rapid detection of pleural space disease, specifically the “TFAST” (thoracic focused assessment with sonography for trauma) procedure. It does, however require practice to be competent in its use.
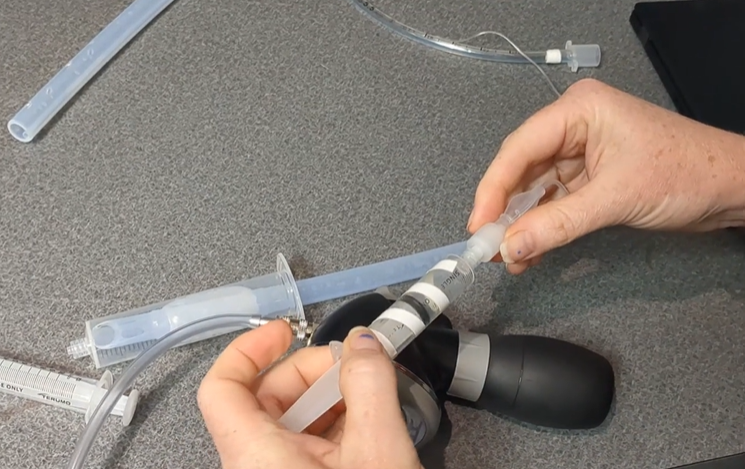
When radiographs are not suitable, the unstable patient may benefit from thoracocentesis, which can be both diagnostic and therapeutic. The equipment needed for this procedure includes clippers, scrub, sterile gloves, a 10-60ml syringe, 3-way stop-cock, butterfly catheter or needle and extension tubing. The site preparation and eventual needle placement for a patient suspected of a pneumothorax is on the dorsal 1/3 of the thorax between the 7th-10th intercostal spaces. The needle is inserted cranial to the rib to avoid the intercostal artery, vein, and nerve located caudal to each rib. Air is aspirated until negative pressure is obtained.
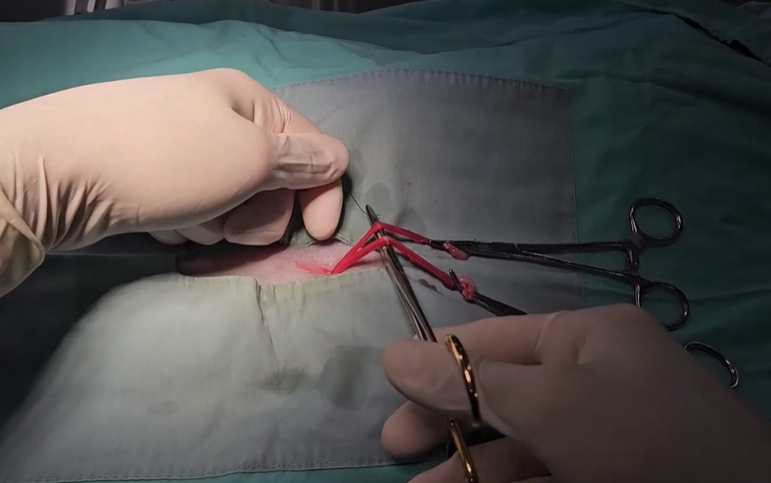
A chest tube is indicated when thoracocentesis needs to be repeated multiple times over a short period of time or when the clinician cannot achieve negative pressure on simple thoracocentesis. Large bore chest tubes require sedation or general anesthesia. Smaller bore chest tubes are also available, placed via the modified seldinger technique with the patient awake or receiving local analgesia. Equipment required for chest tube placement includes clippers, surgical scrub, surgical blade, local analgesia, suture material, the thoracostomy tube, 3-way stop-cock and syringes for initial aspiration. The chest tube can be used intermittently or attached to a suction device for continuous suction. The technique for chest tube placement will depend on the type of tube used, including surgical and trocar methods for the larger bore tubes or the modified seldinger technique for the smaller bore tubes. Like the thoracocentesis, surgical preparation of the site between the 7th-10th intercostal spaces is recommended.
Pulmonary Contusions
Pulmonary contusions result from blunt or crushing trauma and are one of the most common problems associated with thoracic trauma, seen in approximately 50% of all thoracic injuries. Thoracic trauma leads to blood within the alveoli, ventilation/perfusion mismatch, increased pulmonary shunt fraction, and loss of lung compliance. Hypoxemia, increased work of breathing, and hypercarbia, are the physiologic results.
Physical examination findings may include tachypnea, hemoptysis, increased respiratory effort, and harsh lung sounds or crackles on auscultation. Radiographically, there may not be evidence of pulmonary contusions on presentation, delayed anywhere from 12 to 48 hours following trauma. When present, contusions appear radiographically as dense patchy, interstitial to alveolar disease.
As discussed above, initial fluid resuscitation must be started with caution as large volumes of rapidly administered fluid can exacerbate the fluid within the alveolar space with increased vascular permeability, worsening the hypoxemia. If radiographs have evidence of pulmonary contusions, the astute clinician should carefully look for concurrent abnormalities including pneumothorax and/or rib fractures. Additional diagnostic findings may include hypoxemia on pulse oximetry or arterial blood and an increased A-a gradient.
There is no specific medication or reversal therapy for pulmonary contusions. Common supportive care measures include oxygen supplementation, judicious IV fluid therapy, and analgesics. Although evidence is lacking, low dose diuretic therapy has been described anecdotally (furosemide, 0.5 to 1 mg/kg IV intermittently or CRI) in the treatment of pulmonary contusions.
Fractured Ribs
Rib fractures result in discomfort and reduced diaphragmatic and chest wall motion. More specifically, the reduced chest wall motion and pulmonary expansion results in decreased oxygenation, ventilation, and atelectasis of the lungs. Rib fractures should be a clue to the astute clinician that severe thoracic trauma occurred prompting careful evaluation for additional injuries such as pulmonary contusions or a pneumothorax. Physical examination findings may include an increased respiratory rate with shallow respirations, subcutaneous emphysema, palpation of crepitus over the fracture site, and/or conformational changes of the chest wall.
Treatment of rib fractures consists of treating concurrent injuries such as pulmonary contusions, oxygen therapy if hypoxemia exists, and pain management with local or systemic analgesia.
Flail chest
A flail chest is a more severe manifestation of the simple rib fracture. A flail segment occurs when 2 or more ribs are fractured at the junction of ribs and the sternum producing a paradoxical movement of the flail segment. On inspiration, the chest wall normally expands. With a flail segment, the negative intrapleural pressure causes the flail segment to collapse inward during inspiration. On expiration, the chest wall normally collapses. With a flail segment, the intrapleural pressure becomes less negative and the flail segment moves outward on expiration. Abnormal chest movement and the accompanying pain from the fractures themselves result in decreased oxygenation, ventilation, and pulmonary atelectasis.
Treatment consists of placing the patient in lateral recumbency with the flail side down, minimizing movement of the flail segment and reducing the associated fracture discomfort. Pain management includes local nerve blocks and systemic opioid analgesia. Surgical stabilization of the flail segment may also be indicated.
Hemothorax
A hemothorax is defined as an accumulation of blood in the pleural space. This is uncommon following trauma. If present, the amount of blood loss into the pleural space is usually minimal and does not contribute significantly to respiratory compromise. If a large amount of hemorrhage into the pleural space is documented, there should be an increased suspicion for rupture of a large vessel. More common causes for a hemodynamically insignificant hemothorax include laceration of pulmonary or intercostal vessels and/or lung laceration by a fractured rib.
The diagnosis of hemothorax is often be made on physical examination with signs including dyspnea, tachypnea, dull lung sounds ventrally, muffled heart sounds, and signs of hypovolemic or hemorrhagic shock. Thoracocentesis confirms the diagnosis when hemorrhagic fluid is obtained during aspiration with a PCV and TP of the effusion similar to that of the PCV and TP of the peripheral blood.
Treatment of a traumatic hemothorax may include diagnostic and therapeutic thoracocentesis, intravenous crystalloid or synthetic colloid therapy and blood products, notably whole blood or packed red blood cell transfusions. Autotransfusion can be considered if blood products are not available.
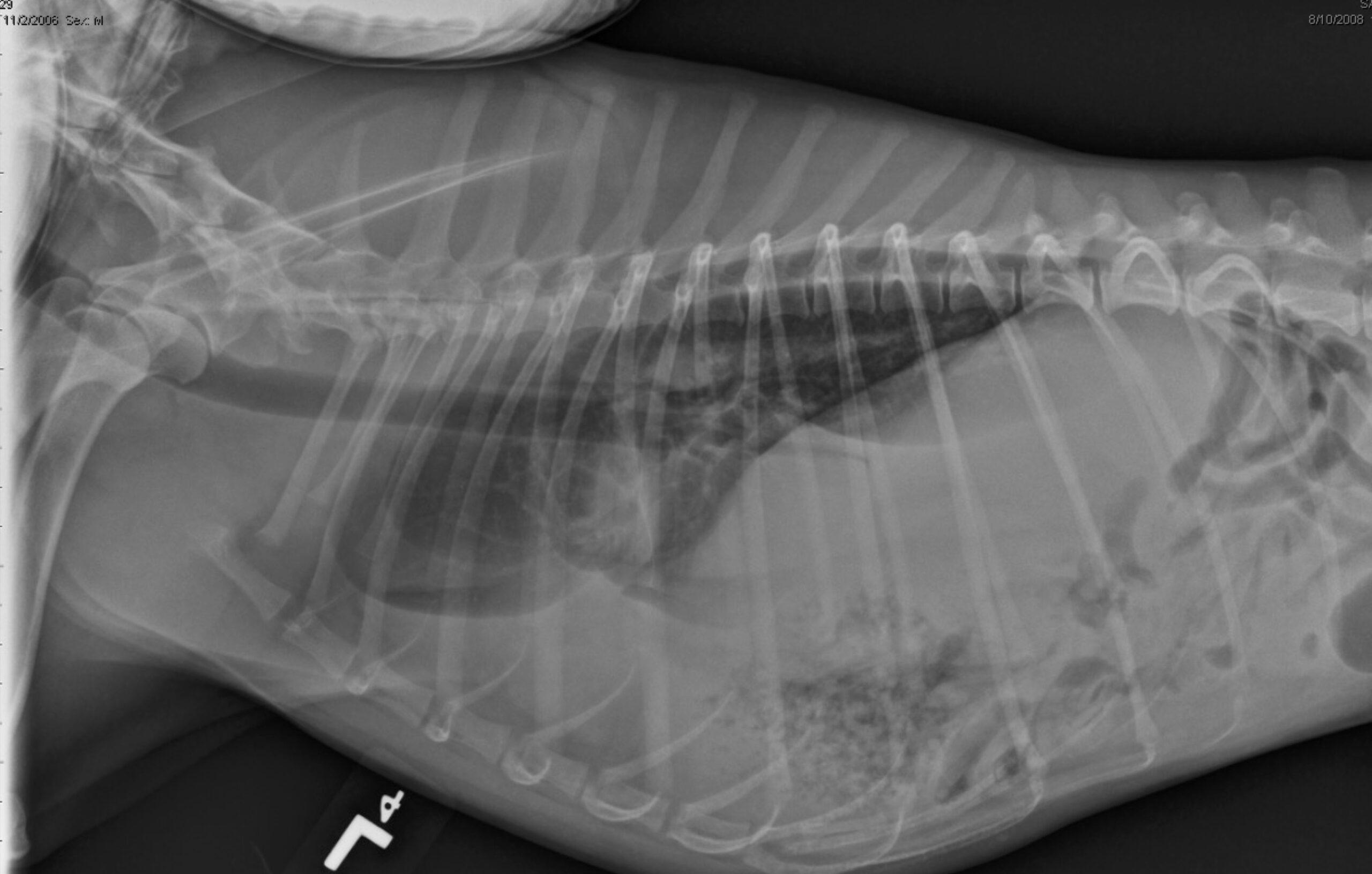
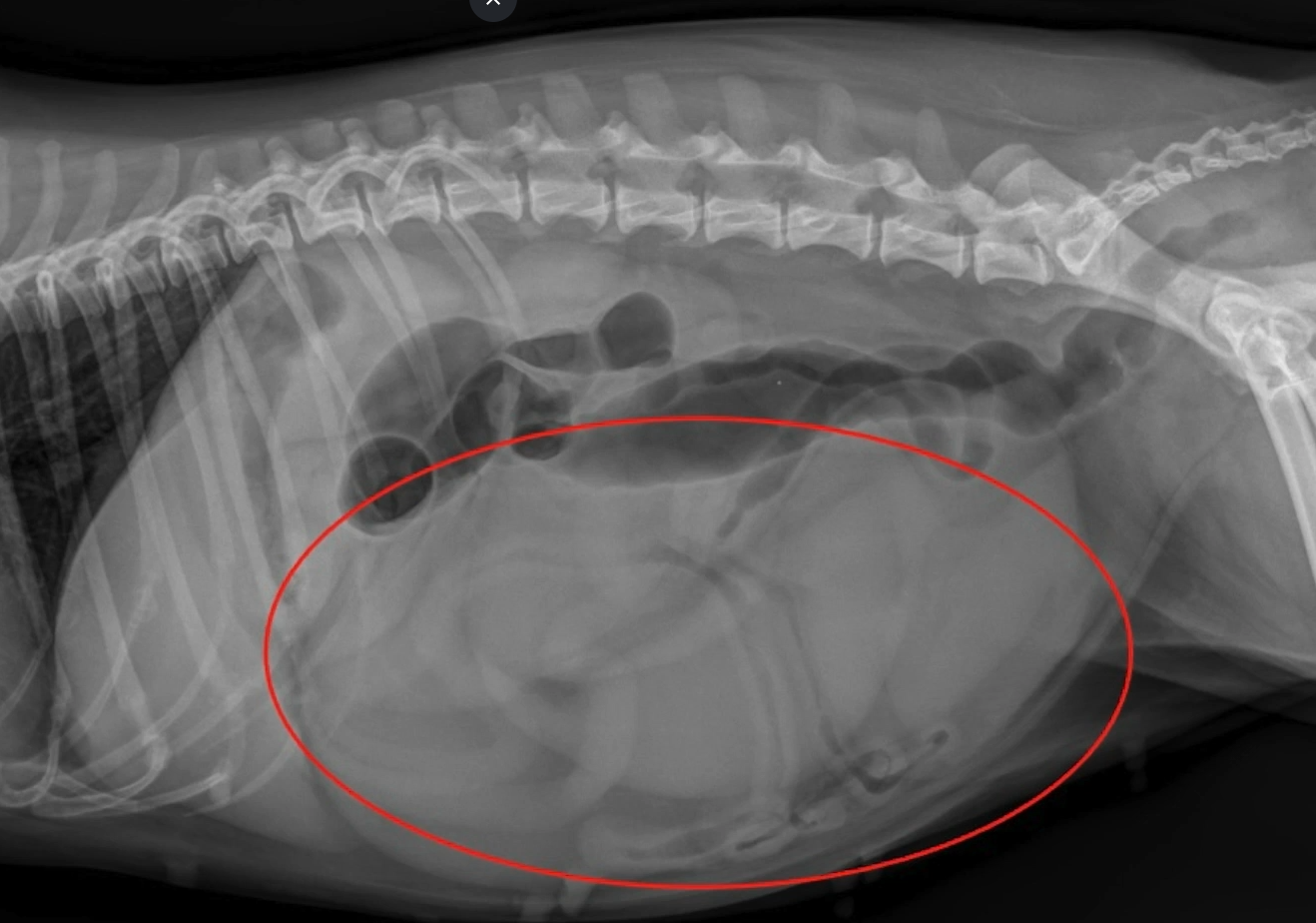
Diaphragmatic Hernia
Diaphragmatic hernia is defined as disruption of the diaphragm, allowing displacement of abdominal organs into the thoracic cavity. Diaphragmatic hernia occurs most often as a result of blunt trauma where intra-abdominal pressure is suddenly increased causing rupture of the diaphragm. The resulting herniation of abdominal contents can range from a single organ or component of an organ (such as a single liver lobe) to almost all the abdominal contents moving cranially through the diaphragmatic rent into the chest cavity. The result is restriction of lung expansion and respiratory distress.
The diagnosis of diaphragmatic hernia can be made with physical examination findings and radiographic abnormalities. Clinical signs of diaphragmatic hernia depend upon the type and number of organs within the chest cavity as well as associated abnormalities such as fluid in the pleural space or pulmonary contusions. Examination findings may be mild and include a slight tachypnea or may result in severe dyspnea, dull lung sounds, muffled heart sounds, borborygmi from the stomach or intestines ausculted in the thorax, abnormal percussion, and a tucked/empty abdomen on palpation. Thoracic radiographs are often diagnostic with the presence of abdominal organs in the thorax.
Abdominal Trauma
The ultimate goal in diagnosis and therapy of the abdominal trauma patient is to determine if the diagnosis lends itself to medical therapy or if surgical intervention is warranted. Importantly, trauma patients require an overall evaluation as patients may not only present with isolated abdominal injury, but also suffer from a polytrauma pattern (traumatic brain injury, thoracic trauma, etc.). For this reason, on presentation, a triage history should be taken while a rapid triage examination / evaluation is occurring. Major body systems for the triage examination include the respiratory system (e.g., airway, breathing), cardiovascular system (e.g., circulation), and neurologic system (e.g., dysfunction). Failure to recognize an abnormality in any of these systems can result in immediate life-threatening deterioration of the patient.
With this information, I try to place them into one of three categories:
- Nonsurgical (medical)
- Emergent
- Critical
Surgery is almost always indicated for penetrating trauma; however, surgery may not be indicated for blunt trauma.
Nonsurgical patients:
Examples of nonsurgical (medical) patients include those diagnosed with traumatic pancreatitis and a cardiovascularly stable traumatic hemoabdomen.
Emergent surgical patients:
Examples of emergent surgical patients include those diagnosed with an unstable hemoabdomen or uroabdomen. These patients are surgical candidates but tolerate medical therapy for stabilization prior to anesthesia and surgery.
Critical surgical patients:
Critical surgical patients, as compared to the previous two groups, require immediate emergency abdominal surgery. Examples of critical patients include mesenteric torsion, septic peritonitis, and uncontrolled hemorrhage. While they may require some degree of medical therapy prior to anesthesia and surgical evaluation, rapid assessment and treatment is needed and delay in surgical correction will increase morbidity and mortality.
The seasoned clinician has mastered the art of multi-tasking, and while taking the history and performing the examination, is often barking out orders to the support staff! To assess the patient, you may ask for:
- Placement of peripheral IV catheter(s)
- Intermittent or continuous ECG for cardiac monitoring
- Pulse oximetry
- Blood pressure
- PCV/TP/BG/Lactate/Electrolytes/Azo
Based on your examination and initial diagnostic results, primary treatments may include:
- Intravenous Fluid therapy to correct hypovolemia and improve perfusion.
- Administration of balanced isotonic crystalloids (10-30ml/kg) in incremental boluses
- Administration of synthetic colloids (hydroxyethyl starch 3-5 ml/kg) in incremental boluses
- Supplemental oxygen – if there is labored breathing or abnormal perfusion
- Analgesic therapy
- Opioid therapy is most commonly used (SEE OPIOD CHART).
- Nonsteroidal anti-inflammatory medication should be used with caution until the underlying cause has been established. Hypoperfusion, gastrointestinal compromise, and the potential need for anesthesia and surgery limit the usefulness of NSAIDS in this situation.
SECONDARY SURVEY
Secondary survey and additional diagnostics may include:
- Complete blood count
- Evaluation of white blood cell count, red blood cell count, and platelet count
- Serum biochemical profile
- Evaluation of important organ values, blood glucose, and electrolytes
- Coagulation profile
- PT, PTT, Platelet count
- Urinalysis and urine sediment
- Evaluation of the urine specific gravity, presence of bacteria, or other abnormalities.
- Diagnostic imaging
- Radiography
- Diaphragmatic Hernia
- Peritonitis
- Loss of abdominal detail due to increased peritoneal fluid
- Abdominal ultrasound
- Peritoneal effusion
- Diaphragmatic Hernia
- Abdominocentesis
- Ultrasound guided or 4-quadrant technique
- DPL
- When there is a small volume effusion or ultrasound is not available, a diagnostic peritoneal lavage (DPL) may be necessary to collect samples for evaluation.
- Cytology of the effusion / Effusion Analysis
- Septic – presence of degenerate neutrophils / intracellular bacteria / Food material
- Measurement of lactate and glucose (compared to plasma in evaluation of sepsis) – An effusion to serum glucose concentration difference >1.1 mmol/L [>20 mg/dL] is highly suspicious of a septic effusion
- Measurement of creatinine and potassium – Peritoneal effusion-to-serum potassium concentration ratios of 1.4:1 and 1.9:1 are considered diagnostic for uroabdomen in dogs and cats, respectively
- Measurement of bilirubin (compared to plasma in evaluation of biliary tract rupture) An effusion to serum bilirubin concentration difference >2mg/dL is highly suspicious of a bile peritonitis
- Radiography
Indications for emergency surgical intervention include:
- Inability to medically stabilize intrabdominal hemorrhage
- Free gas on abdominal radiographs (provided they were taken prior to abdominocentesis and there is no recent abdominal surgery)
- Cytological evidence of intracellular bacteria or plant/food material in the abdominal fluid
- Elevated creatinine and potassium levels compared to peripheral serum levels
- Elevated bilirubin levels higher compared to peripheral serum levels
- Penetrating abdominal injury
How soon should surgery be performed once the diagnosis is made?
This depends on two factors:
- How stable is the patient?
- What is the underlying diagnosis?
Most patients presenting with abdominal trauma (or polytrauma) will require some degree of stabilization prior to anesthesia and surgery. Hypovolemia and acid-base or electrolyte abnormalities are common findings in patients that present following trauma. These should be addressed prior to induction of anesthesia. Clinical judgment is needed to determine the appropriate balance between stabilization before surgery and the time that passes before the patient is placed under anesthesia to surgically correct the problem.
Along with fluid therapy, electrolyte correction, and potential surgical correction, other therapies consider include:
Antibiotics
- Translocation of gram positive and gram-negative aerobes and anaerobes may occur following a period of poor perfusion and alteration to the integrity of the gastrointestinal tract.
Common antibiotic broad-spectrum combinations the author uses includes:
- Cefazolin 20-30mg/kg IV q8-12h or Ampicillin 22 mg/kg IV q8hr
- Metronidazole 10 mg/kg IV q12 hr
- Baytril 10-15mg/kg IV q24h (canine)
- Ampicillin/sulbactam 20-30 mg/kg IV q 8h
- Baytril 10-15mg/kg IV q24h (canine)
- Metronidazole 10 mg/kg IV q12 hr
- Clindamycin 8-11mg/kg IV q8-12h
- Cefotaxime 30-50mg/kg IV q6h
Ultimately, the prognosis for patients with abdominal trauma will depend on the underlying disease process. Rapid evaluation and treatment of life-threatening complications such as hypovolemic shock will decrease morbidity and give the astute clinician time to obtain the diagnosis to best assist the pet parents in helping their pet.
Gastrointestinal Protectants and Associated Medications:
| Medication | Drug Class | Dose Range | Frequency | Route |
| Chlorpromazine | α2 and D2 Antagonist | 0.1–0.5 mg/kg | Q8 | SQ, IM, Rectal Suppository |
| Dolasetron | 5-HT3 Antagonist | 0.5–1.0 mg/kg | Q12-24h | IV, SQ |
| Maropitant | NK-1 Antagonists | 1 mg/kg 2 mg/kg |
Q24 Q24 |
SQ PO |
| Metoclopramide | D2 Antagonist | 0.2–1 mg/kg 1–2 mg/kg/day |
Q6 CRI |
PO, SQ, IM
IV CRI |
| Ondansetron | 5-HT3 Antagonist | 0.1–0.3 mg/kg | Q6-24h | PO IV |
| Prochlorperazine, | α2 and D2 Antagonist | 0.1–0.5 mg/kg | Q8 | SQ, IM, Rectal Suppository |
Opioid Drug Chart
| Medication | Dose Range | Frequency | Route |
| Buprenorphine | 0.01-0.02 mg/kg | Q4-6h | SQ, IM, IV |
| Hydromorphone | 0.05–0.2 mg/kg | Q4-6h | SQ, IM, IV |
| Fentanyl | 25 mcg patch < 10 kg 50 mcg patch 10–20 kg 75 mcg patch 20–30 kg 100 mcg patch >30 kg |
Q3–4 days Onset of effect 12–24 hrs after application |
Dermal |
| Fentanyl | 3–10 mcg/kg/hr (2-5 mcg/kg initial IV bolus) |
IV CRI | IV CRI |
| Morphine | 0.5–2.0 mg/kg | Q4-6h | SQ, IM |
| Methadone | 0.1-0.4 mg/kg SC, IM, IV | Q6h | SQ, IM, IV |
References
1) Bonczynski JJ, Ludwig LL, Barton LJ, et al: Comparison of peritoneal fluid and peripheral blood pH, bicarbonate, glucose, and lactate concentration as a diagnostic tool for septic peritonitis in dogs and cats, Vet Surg 32:161, 2003.
2) Boysen SR, Rozanski EA, Tidwell AS, et al. Evaluation of a focused assessment with sonography for trauma protocol to detect free abdominal fluid in dogs involved in motor vehicle accidents. J Am Vet Med Assoc. 2004;225(8):1198–1204.
3) Boysen SE, Rozanski EA, et al. Evaluation of a focused assessment with sonography for trauma protocol to detect free abdominal fluid in dogs involved in motor vehicle accidents.Journal of the American Veterinary Medical Association 2004;225(8):1198–1204.
4) Bracken MB, Shepard MJ, Collins WF, et al. A randomized, controlled study of methylprednisolone or naloxone in the treatment of acute spinal-cord injury. N Engl J Med1990;322: 1405-1411.
5) Campbell V, et al. Pulmonary function, ventilator management, and outcome of dogs with thoracic trauma and pulmonary contusions: 10 cases (1994-1998).J Am Vet Med Assoc. 2000 Nov 15;217(10):1505-9.
6) Cockshutt JR. Management of fracture-associated thoracic trauma. Vet Clin North Am, Small Anim Pract. 1995; 25: 5, 1031-1046.
7) Chestnut RM, Marshall LF, Klauber MR et al. The role of secondary brain injury in determining outcome from severe head injury. J Trauma 1993;34: 216-222.
8) Coughlan AR. Secondary injury mechanisms in acute spinal cord trauma. J Sm Anim Pract 1993;34: 117.
9) Crowe D, Devey J. Assessment and management of the hemorrhaging patient. Vet Clin North Am [Small Anim Pract] 24:1095, 1994
10) Crowe DT. Diagnostic abdominal paracentesis and lavage in the evaluation of abdominal injuries in dogs and cats: clinical and experimental investigations. J Am Anim Hosp Assoc 168:700, 1976
11) Dewey CW. Emergency management of the head trauma patient. Vet Clin North Am Small Anim Pract 2000;30: 207-223.
12) Dewey CW. Brain Trauma. In: Wingfield WE, Raffe MR, editors. The Veterinary ICU Book. Jackson Hole, WY: Teton New Media Press; 2002. pp. 911-920.
13) Dewey CW. Myelopathies: Disorders of the Spinal Cord. In: Dewey CW, editor. A Practical Guide to Canine and Feline Neurology. Ames, IA: Iowa State Press; 2003. pp. 277-336.
14) Franks JN, Howe LM. Evaluating and managing acute abdomen. Vet Med 2000; 95(1): 56-69.
15) Gibson TW, et al. Perioperative survival rates after surgery for diaphragmatic hernia in dogs and cats: 92 cases (1990-2002).J Am Vet Med Assoc. 2005 Jul 1;227(1):105-9.
16) Gordon PN, Dunphy E, Mann F. A traumatic emergency: handling patients with head injuries. Vet Med. 2003;98(9):788–798.
17) Gordon LE, Thacher C, Kapatkin A. High-rise syndrome in dogs: 81 cases (1985-1991). J Am Vet Med Assoc. 1993; 202: 1, 118-122.
18) Herold L, Devey J, Kirby R, Rudloff E. Clinical evaluation and management of hemoperitoneum in dogs. J Vet Emerg Crit Care 2008 18(1):40-53)
19) Hopkins AL. Head trauma. Vet Clin North Am Small Anim Pract 1996;26: 875-889.
20) Kirby R, Rudloff E. Acute abdomen. In Morgan R (ed) Handbook of Small Animal Medicine. (3rd ed)
21) Kirby BM. Spinal fracture / luxation. Vet Clin North Am Small Anim Pract 1995;25: 1149-1173.
22) Lisciandro GR. Abdominal and thoracic focused assessment with sonography for trauma, triage, and monitoring in small animals. J Vet Emerg Crit Care (San Antonio). 2011 Apr;21(2):104-22.
23) Macintire DK. The acute abdomen-differential diagnosis and management. Semin Vet Med Surg (Small Animal) 1988; 3(4): 302-310.
24) Mann FA. Acute abdomen: Evaluation and emergency treatment. In Bonagura JD (ed). Kirk’s Current Veterinary Therapy XIII. Philadelphia: WB Saunders CO; 2002. pp. 160-164.
25) Mathews, K. Management of pain. Vet Clin North Am [Small Anim Pract] 30:4, 2001
26) Muizelaar JP, Marmarou A, Ward JD, et al. Adverse effects of prolonged hyperventilation in patients with severe head injury: a randomized clinical trial. J Neurosurg 1991;75: 731-739.
27) Platt SR, Radaelli ST, McDonnelll JJ. The prognostic value of the modified Glasgow coma scale in head trauma in dogs. J Vet Intern Med 2001;15: 581-584.
28) Powell, LL Rozanski EA, Tidwell AS, Rush, JE. A retrospective analysis of pulmonary contusion secondary to motor vehicular accidents in 143 dogs: 1994-1997. J Vet Emerg Crit Care. 1999; 9(3), 127-136.
29) Proulx J, Dhupa N. Severe Brain Injury. Part I. Pathophysiology. Comp Cont Ed Pract Vet 1998;20: 897-905.
30) Proulx J, Dhupa N. Severe Brain Injury. Part II. Therapy. Comp Cont Ed Pract Vet 1998;20: 993-1005.
31) Rizzi TE, Cowell RL, Tyler RD, Meinkoth JH. Effusions; abdominal, thoracic, and pericardial fluid. In Diagnostic Cytology and Hematology of the Dog and Cat, ed 3. Mosby, St Louis, 2008, pp 235-255.
32) Rudloff E. Abdominocentesis and Diagnostic Peritoneal Lavage. In Ettinger S, Feldman E, Textbook of Veterinary Internal Medicine (4th ed) 2005; pp269-270.
33) Saxon W. The acute abdomen. Vet Clin North Am Small Anim Pract 1994; 24(6): 120
34) Serrano S, Boag A. Pulmonary contusions and hemorrhage. In: Silverstein DC and Hopper K, eds. Small Animal Critical Care Medicine. St. Louis, MO: Elsevier; 2009:105–110.
35) Shores A. Spinal Trauma: Pathophysiology and management of traumatic spinal injuries. Vet Clin North Am Small Anim Pract 1992;22: 859-887.
36) Spackman CJA, Caywood DD, Feeney DA, Johnston GR. Thoracic wall and pulmonary trauma in dogs sustaining fractures as a result of motor vehicle accidents. J Am Vet Med Assoc. 1984; 185: 9, 975-977.
37) Streeter EM, McDonnell JJ, O’Toole TE et al. Prospective evaluation of head trauma in 24 dogs: modified Glasgow coma scale, animal trauma triage score, computed tomography findings and outcome, in Proceedings. 9th International Veterinary Emergency and Critical Care Symposium 2003; 774.
38) Syring RS, Otto CM, Drobatz KJ. Hyperglycemia in dogs and cats with head trauma: 122 Cases (1997-1999). J Am Vet Med Assoc 2001;218: 1124-1129.
39) Whitney WO, Mehlhaff CJ. High-rise syndrome in cats. J Am Vet Med Assoc. 1987; 191: 11, 1399-1403.
Only VETgirl members can leave comments. Sign In or Join VETgirl now!



Great information
More like this
Good blog
Very helpful
Good read