





August 2023
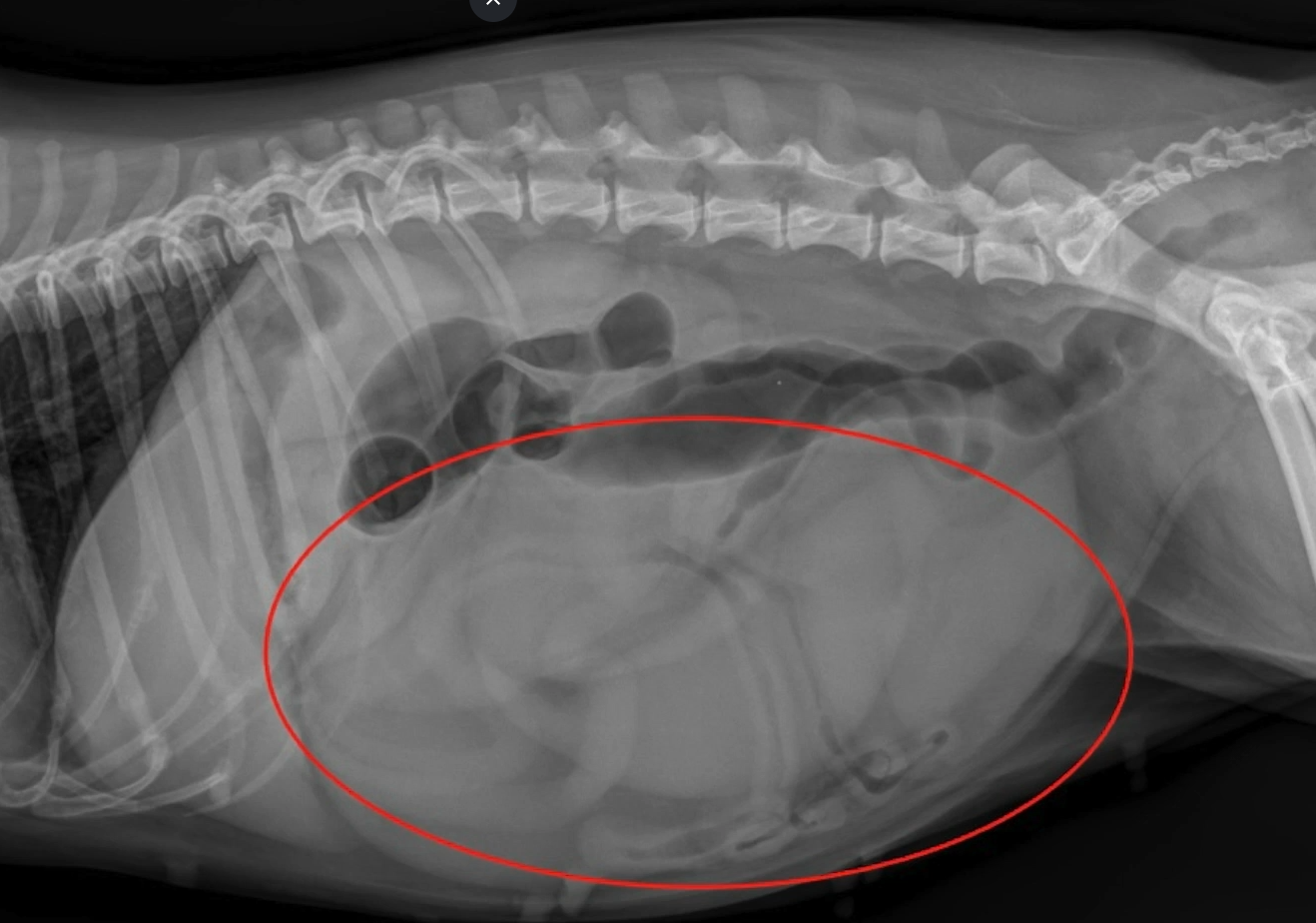
In today’s VETgirl sponsored online veterinary continuing education blog, guest blogger Dr. David C. Twedt DVM, DACVIM discusses treatment of acute canine pancreatitis (ACP). If you’re about to see a dog that presents in that “classic” prayer position, with vomiting, abdominal pain, and dehydration, tune in to learn what’s new when it comes to treatment!
Treatment of Acute Canine Pancreatits: Are You Ready for a Paradigm Shift? with Dr. David C. Twedt
By Dr. David C. Twedt DVM, DACVIM (Small Animal Internal Medicine), Fort Collins, CO
Vomiting again? Worried about pancreatitis? This can be a hard disease to diagnose and understand sometimes, especially when the exact mechanism is unclear for targeting treatment. What do we know?
What is your first thought when presented with a vomiting Schnauzer? What about the Labrador who got into last night’s garbage? If you’re thinking pancreatitis, you’re probably right. In fact, pancreatitis is likely more common than previously thought (Cridge, Lim, Algul, & JM, 2022).
Exact prevalence is unknown but necropsy studies, insurance data, and clinical experience can give insight as to this common disease. In 2004, a total of 73 pancreata from dogs presented for postmortem examination. 47 of the pancreata showed histological evidence of pancreatitis (Watson, et al., 2007). When reviewing pet insurance data, gastrointestinal disorders is the most commonly reported disease (Embrace Pet Insurance, n.d.). Finally, it is estimated that every US veterinarian sees at least 4 acute canine pancreatitis cases per month or 48 annually (Data on file, Ishihara Sangyo Kaisha, LTD., 2018).
The exact pathophysiology of canine pancreatitis is unclear. In veterinary medicine, a long-held belief that autodigestion of the pancreas from prematurely activated pancreatic zymogens (enzyme precursors) is to blame…but now what we know is that the mechanism is unclear (Cridge, Lim, Algul, & JM, 2022)
We also know that pancreatitis can progress from mild with no recognizable tissue necrosis to severe with acinar necrosis, inflammation, and injury of extra-pancreatic organs in which morbidity and mortality are higher (Cridge, Lim, Algul, & JM, 2022).
So, what is causing pancreatitis? We know that the pathobiological process underlying necrotizing pancreatitis results from a leukocyte attraction into the pancreas and adjacent tissues. The hallmark of pancreatitis is neutrophilic mediated inflammation that releases additional inflammatory mediators potentiating pancreatic damage. It is now considered that inflammation plays a significant role in the pathogenesis of pancreatitis rather than autodigestion (Cridge, Lim, Algul, & JM, 2022).
Treatment: What can we learn from human medicine?
For humans suffering from acute pancreatitis, there is a reported important short 48-hour therapeutic window for successful management of acute pancreatitis (Mayerle, Simon, & Lerch, 2004). Survival rates decreased and complication rates increased if treatment was delayed beyond this initial period. Rapid fluid resuscitation is the first aid line to minimize or prevent compromise to the microcirculation of the pancreas, preventing more severe necrotizing pancreatitis cases. We can apply this to the management of canine pancreatitis in that rapid recognition and early therapy is imperative for improved outcomes.
An ACVIM forum from years ago identified the top four most important therapies by a group of veterinary gastroenterologists (Multiple, 2006). This included fluid therapy, analgesics, antiemetics, and nutritional therapy. Other therapies were suggested to have lesser importance including antibiotics, antacids, corticosteroids, and surgery. Therapies that have been mentioned but lack adequate studies in the dog are pancreatic enzyme replacement, dopamine, antioxidants, hyperbaric oxygen, and cold laser therapy.
A new Break-through in Pancreatitis Therapy (Take the “ITIS” out of Pancreatitis)
No matter the etiology, we all know that when pancreatitis progresses from the mild edematous form to the more severe necrotizing form, the disease severity increases. But when a patient presents with clinical signs of pancreatitis, it is often not possible to predict the outcome. You never know where it could go. Even mild cases can progress rapidly. This is why early intervention is needed. The recruitment and activation of inflammatory cells results in local release of proinflammatory factors with recruitment of neutrophils into the inflammatory tissues. This is a multistep process called extravasation. Leukocyte sequestration begins with activation and adhesion to the microvascular endothelial surfaces and culminates with transmigration of neutrophils across the endothelial barrier into the tissues. As neutrophils are called to the site of activation, they begin to slow and roll along the vascular endothelium. ICAM-1 (endothelial cell surface adhesion molecule – 1) regulates this barrier and functions in interactions and migrations of neutrophils into inflamed areas. The leukocyte function-associated antigen-1 (LFA-1) receptor on the leukocyte surface plays a key role in this binding process to ICAM-1. Inflammatory cytokines activate the LFA-1 on the neutrophil through an inside out signaling that unfolds the LFA-1 receptor allowing it to attach to ICAM-1 and migrate into inflamed tissues.
There has been considerable research in medicine over recent years looking for drugs to inhibit neutrophil adhesion properties and prevent infiltration into the pancreas to prevent inflammation of tissues. Specifically, in a mouse study, the role of ICAM-1 and its counter receptor LFA-1 in acute pancreatitis models found that blocking this pathway is an important window of opportunity in the treatment of acute pancreatitis. Identified by a veterinary researcher in Japan several years ago, fuzapladib sodium was created as an LFA-1 inhibitor for acute canine pancreatitis. It was first tested in vivo on a canine experimental pancreatitis model that used bile infusion into the pancreatic duct to cause pancreatitis. This had a 50% mortality rate in untreated dogs while the fuzapladib treated group had no mortality. The next trial was a multi-center trial in Japan that found dogs treated with acute pancreatitis had greater improvement scores in both clinical signs and c-reactive protein levels than the untreated counterparts. The drug (BRENDA™) then became commercially available in Japan and is now widely used by Japanese veterinarians to treat acute canine pancreatitis cases. The following adverse events were reported voluntarily during post-approval use of the product in dogs in Japan: facial and tongue swelling, collapse, and seizure. These adverse events occurred within 24 hours of administration. This formulation has the same active ingredient and concentration that is found in PANOQUELL®-CA1 (fuzapladib sodium for injection).
PANOQUELL®-CA1 is now conditionally approved by the FDA pending a full demonstration of effectiveness under application number 141-567. It is indicated for the management of clinical signs associated with acute onset of pancreatitis in dogs and available through Ceva Animal Health in the United States. PANOQUELL®-CA1 (a selective inhibitor of LFA-1) has anti-inflammatory effects through its ability to inhibit activation of LFA-1, resulting in inhibition of inflammatory cell adhesion and migration into sites of tissue injury and inflammation. These anti-inflammatory properties are thought to limit pancreatic lesion expansion and help prevent complications such as multi-organ failure. Based on the data submitted by the sponsor for the conditional approval of PANOQUELL®-CA1, FDA determined that the drug is safe and has a reasonable expectation of effectiveness when used according to the labeling.
The effectiveness of fuzapladib sodium was demonstrated in a well-controlled pilot field study. Dogs treated with fuzapladib sodium had a statistically significant reduction in Modified Canine Activity Index (MCAI) scores compared to control. In this study, PANOQUELL-CA1 was administered safely with other supportive care treatments including anti-emetics and pain control. The most common adverse reactions included anorexia, digestive tract disorders, respiratory tract disorders, and hepatopathy and jaundice.
PANOQUELL®-CA1 is administered at a dose of 0.4 mg/kg IV once daily for 3 consecutive days. The drug comes in a multiuse vial (14mg) as a lyophilized powder that is reconstituted with a sterile diluent. Once reconstituted, the drug remains stable in the refrigerator for 28 days. Minimal adverse effects reported in a few cases include gastrointestinal, transient hypertension, or injection site inflammation. It is a violation of Federal law to use this product other than as directed in the labeling.
When should we use PANOQUELL®-CA1? Learning from human medicine, we know early intervention helps these patients. Looking at the mechanism of action of the medication, the most beneficial therapeutic window to prevent further neutrophilic infiltration to the pancreas is as soon as you see clinical signs and have an indication clinically on your physical exam for acute canine pancreatitis.
Follow up: You’ve successfully treated pancreatitis. What now? Guidance on post pancreatitis treatment
Guidelines have not been specifically established but here is a good practice from this internist:
- Place on LOW FAT DIET
- Antioxidant therapy such as vitamin E at 10 IU/kg/day AND SAMe (s-adenosylmethionine or other liver support medications such as SAMeLQ).
- If at recheck in 2-3 weeks:
- Pet is clinically stable:
- Repeat Spec CPL or Precision PSL: if normal, then RECOVERED!
- Gradually return to complete balanced diet
- Correct any risk factors
- Discontinue antioxidant therapy.
- Pet is clinically normal, but Spec CPL or Precision PSL is ABNORMAL:
- Suspect low grade chronic pancreatitis
- Continued diet of LOW FAT
- Continue antioxidant therapy
- Pet is clinically stable:
- Remember, for chronic pets, REMIND owners that they can have an ACUTE FLAIR at any time. Try and manage or avoid all potential risk factors (hyperlipidemia, fatty meals, etc.) and address any lingering complications.
*IMPORTANT SAFETY INFORMATION: The safe use of PANOQUELL®-CA1 has not been evaluated in dogs with cardiac disease, hepatic failure, renal impairment, dogs that are pregnant, lactating, intended for breeding or puppies under 6 months of age. PANOQUELL®-CA1 should not be used in dogs with a known hypersensitivity to fuzapladib sodium. PANOQUELL®-CA1 is a highly protein bound drug and its use with other highly protein bound medications have not been studied. The most common side effects in the pilot field study were anorexia, digestive tract disorders, respiratory tract disorders and jaundice. PANOQUELL®-CA1 is not for use in humans. Limited data is available on the potential teratogenic effects of fuzapladib sodium. Therefore, anyone who is pregnant, breast feeding, or planning to become pregnant should avoid direct contact with PANOQUELL®-CA1. For additional information on the use of PANOQUELL®-CA1, please refer to the package insert.
References
- Cridge, H., Lim, S., Algul, H., & JM, S. (2022). New insights into the etiology, risk factors, and pathogenesis of pancreatitis in dogs: Potential impacts on clinical practice. J Vet Intern Med, 36(3), 847-864. doi:10.1111/jvim.16437
- (2018). Data on file, Ishihara Sangyo Kaisha, LTD.
- Mayerle, J., Simon, P., & Lerch, M. (2004). Medical treatment of acute pancreatitis. Gastroenterol Clin North Am, 33(4). doi:10.1016/j.gtc.2004.07.012
- Multiple. (2006). Comparative Gastroenterology Society Program. ACVIM.
- PR Newswire. (n.d.). Retrieved from https://www.prnewswire.com/news-releases/embrace-pet-insurance-releases-top-pet-names-breeds-and-claims-of-2022-301699250.html
- Watson, P., Roulois, A., Scase, T., Johnston, P., Thompson, H., & Herrtage, M. (2007). Prevalence and breed distribution of chronic pancreatitis at post-mortem examination in first-opinion dogs. J of Small Anim Pract., 48(11), 609-618. doi:10.1111/j.1748-5827.2007.00448.x
PANOQUELL® is a registered trademark of Ishihara Sangyo Kaisha, Ltd.
PAN-117-23v1
This VETgirl online veterinary continuing education blog is sponsored by CEVA Animal Health. Please note the opinions in this blog are the expressed opinion of the author(s), and not directly endorsed by VETgirl.
Only VETgirl members can leave comments. Sign In or Join VETgirl now!




hello there,
very good blog post. I am excited to try the new therapy!
So excited about this new treatment option.
Wonderful to have new options for treatment!
Love the Panoquell
I have used this product and it does do exactly what it says it does. Dogs lives have been improved
Good new treatment options